Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline
BMJ 2018; 363 doi: https://doi.org/10.1136/bmj.k5130 (Published 18 December 2018) Cite this as: BMJ 2018;363:k5130©BMJ Publishing Group Limited.
Disclaimer: This infographic is not a validated clinical decision aid. This information is provided without any representations, conditions or warranties that it is accurate or up to date. BMJ and its licensors assume no responsibility for any aspect of treatment administered with the aid of this information. Any reliance placed on this information is strictly at the user's own risk. For the full disclaimer wording see BMJ's terms and conditions: https://www.bmj.com/company/legal-information/

- Kameshwar Prasad, chair, stroke neurologist1,
- Reed Siemieniuk, general internist, methodologist23,
- Qiukui Hao, geriatrician24,
- Gordon Guyatt, general internist, methodologist25,
- Martin O’Donnell, stroke neurologist6,
- Lyubov Lytvyn, patient partnership liaison2,
- Anja Fog Heen, general internist7,
- Thomas Agoritsas, general internist, methodologist28,
- Per Olav Vandvik, general internist, methodologist79,
- Sankar Prasad Gorthi, stroke neurologist10,
- Loraine Fisch, stroke neurologis11,
- Mirza Jusufovic, stroke neurologist12,
- Jennifer Muller, patient partner1314,
- Brenda Booth, patient partner13,
- Eleanor Horton, patient partner15,
- Auxiliadora Fraiz, physiotherapist, nurse,
- Jillian Siemieniuk, nurse16,
- Awah Cletus Fobuzi, patient and carer partner17,
- Neelima Katragunta, vascular surgeon18,
- Bram Rochwerg, methods co-chair, critical care clinician25
- 1Department of Neurology, All India Institute of Medical Sciences, New Delhi, India
- 2Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, Canada
- 3Department of Medicine, University of Toronto, Toronto, Canada
- 4The Centre of Gerontology and Geriatrics, West China Hospital, Sichuan University, Chengdu, China
- 5Department of Medicine, McMaster University, Hamilton, Canada
- 6Deparment of Medicine, NUI Galway, Galway, Ireland
- 7Department of Medicine, Innlandet Hospital Trust-division, Gjøvik, Norway
- 8Division of General Internal Medicine & Division of Clinical Epidemiology, University Hospitals of Geneva, Geneva, Switzerland
- 9Institute of Health and Society, Faculty of Medicine, University of Oslo, Oslo, Norway
- 10Department of Neurology, Kasturba Medical College, Manipal, India
- 11Division of Neurology, Stroke Centre, University Hospitals of Geneva, Geneva, Switzerland
- 12Department of Neurology, Oslo University Hospital Rikshospitalet, Oslo, Norway
- 13Stroke Foundation of Australia
- 14School of Public Health and Social Work, Faculty of Health, Queensland University of Technology, Brisbane, Australia
- 15School of Nursing, Midwifery and Paramedicine, University of Sunshine Coast, Maroochydore, Australia
- 16Peter Lougheed Hospital, Calgary, Canada
- 17Cochrane Consumers Group
- 18Department of Surgery, Stanford University, Stanford, California
- Correspondence to: B Rochwerg rochwerg{at}mcmaster.ca
Abstract
What is the role of dual antiplatelet therapy after high risk transient ischaemic attack or minor stroke? Specifically, does dual antiplatelet therapy with a combination of aspirin and clopidogrel lead to a greater reduction in recurrent stroke and death over the use of aspirin alone when given in the first 24 hours after a high risk transient ischaemic attack or minor ischaemic stroke? An expert panel produced a strong recommendation for initiating dual antiplatelet therapy within 24 hours of the onset of symptoms, and for continuing it for 10-21 days. Current practice is typically to use a single drug
What you need to know
People with high risk transient ischaemic attack or minor ischaemic stroke are at an increased risk of recurrent stroke and death
Aspirin and clopidogrel decrease this risk, even more so when used in combination
We make a strong recommendation for dual antiplatelet therapy (DAPT) with clopidogrel and aspirin to be started within 24 hours in patients who have had a high risk transient ischaemic attack or minor stroke
We make a strong recommendation for DAPT to be continued for 10-21 days, at which point patients should continue with single antiplatelet therapy
DAPT is not to be used for major stroke because of the increased risk of intracranial bleeding in these patients
The recommendations in this clinical practice guideline are based on a linked systematic review1 triggered by a randomised controlled trial published in the New England Journal of Medicine in August 2018.2 This trial and the linked review found that dual antiplatelet therapy (DAPT) with clopidogrel and aspirin (acetylsalicylic acid) during the first 21 days after the index event reduced the risk of recurrent major ischaemic events compared with aspirin monotherapy.
This Rapid Recommendation aims to quickly and transparently translate evidence for working clinicians and their patients in adherence with standards for trustworthy guidelines and the GRADE system.345 A panel free of financial conflicts of interest, and including patients, drafted the recommendations. We have managed intellectual interests.
Box 1 shows all of the articles and evidence linked in this Rapid Recommendation package. The core infographic provides an overview of the absolute benefits and harms for DAPT compared with aspirin monotherapy.
Linked articles in this BMJ Rapid Recommendations cluster
Prasad K, Siemieniuk R, Hao Q, et al. Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline. BMJ 2018;363:j656:k5130. doi:10.1136/bmj.k5130
Summary of the results from the Rapid Recommendation process
Hao Q, Tampi M, O’Donnell M, Foroutan F, Siemieniuk RAC, Guyatt G. Clopidogrel plus aspirin versus aspirin alone for acute minor ischaemic stroke or high risk transient ischaemic attack: systematic review and meta-analysis. BMJ 2018;363:k5108. doi:10.1136/bmj.k5108
Review of all available randomised trials that assessed dual antiplatelet therapy (clopidogrel and aspirin) versus aspirin monotherapy after a high risk transient ischaemic attack or minor stroke
MAGICapp (www.magicapp.org)
Expanded version of the results with multilayered recommendations, evidence summaries, and decision aids for use on all devices
Current practice
Single antiplatelet therapy with aspirin or clopidogrel is an effective intervention for both short and long term secondary prevention of stroke and transient ischaemic attack after an index event. Clinicians sometimes use alternatives of cilostazole or a combination of dipyridamole and aspirin, both referred to for this recommendation as single agent therapy.6789
Aspirin and clopidogrel have synergistic action to inhibit platelet aggregation. So it is plausible that the two drugs together may provide better secondary prevention of stroke than one. However, they are not in widespread use for various reasons:
They are not useful in the long term after stroke—Several large randomised controlled trials (RCTs) have examined if DAPT (aspirin and clopidogrel) is better at preventing recurrent stroke than single agent antiplatelet therapy. However, DAPT was no better than single agent therapy.1011
They are considered too risky after major stroke—Major strokes, as opposed to minor ones, are treated with single agent only because of the higher risk of haemorrhagic transformation.
The balance of benefit and harm is uncertain for short term use after minor stroke or high risk transient ischaemic attack—In the days and weeks after such an event there is an increased risk of a second ischaemic event. This uncertainty in the setting of acute transient ischaemic attacks and minor stroke could have been reduced by the recent RCT.
Table 1 outlines how international guidelines vary. A minority make a weak recommendation or suggestion for short term DAPT. It also shows some international variation in the single agents that are recommended in the long term. The NICE guideline favours clopidogrel over others, and combined aspirin and dipyridamole over aspirin, whereas most guidelines consider all three as equivalent options.
Current recommendations for antiplatelet therapy for secondary prevention of stroke
The ABCD2 score and NIHSS score are typically used to help assess the severity of a transient ischaemic attack or stroke and can help to guide future care. Around 1 in 10 people go on to have a stroke after high risk transient ischaemic attack (box 2). The chance of a further stroke soon after minor stroke is less clear but is likely to be around 10-12% range.
Assessment of severity of transient ischaemic attack and minor stroke and subsequent risk of stroke
Transient ischaemic attack
Severity assessed by ABCD2 score:
Age—1 point if ≥60 years
Blood pressure—1 point if ≥140/90 mm Hg
Clinically—1 point if speech disturbance only, 2 points if unilateral weakness
Duration—1 point if 10 minutes to 1 hour, 2 points if ≥1 hour
Diabetes—1 point if present
Subsequent risk of stroke based on ABCD2 score:
Score 1-3 (low)=1.2% at 7 days
Score 4-5 (moderate)=5.9% at 7 days
Score 6-7 (high)=11.7% at 7 days
Minor stroke
Severity defined as NIHSS score ≤3
Subsequent risk of stroke not well characterised but likely equal to that of a high risk transient ischaemic attack
NIHSS = National Institute of Health Stroke Scale.14 Scale ranges from 0 to 42, based on assessment of 15 measures of motor and sensory function, language and speech production, vision, level of consciousness and attention, and neglect. The elements are summed to provide an overall assessment of stroke severity. A score of 0 to 3 or 4 indicates mild stroke, 5-14 moderate, 15-24 moderately severe, and ≥25 severe.
How this recommendation was created
This guideline was triggered by a randomised controlled trial that compared dual antiplatelet therapy (DAPT, clopidogrel plus aspirin) with aspirin monotherapy given within 12-24 hours of symptom onset in patients with high-risk transient ischaemic attack or minor stroke.2 This added to a previous DAPT trial published in 2013.15 The Rapid Recommendations team thought that the results had the potential to change practice.
The scope of the recommendation and the patient-important outcomes were defined by an international guideline panel consisting of three patients with lived experience of stroke, one adult who cared for someone with a stroke, five stroke neurologists, one vascular surgeon, one health research methodologist, five general internists (four who are also methodologists), one nurse, one physiotherapist, and one critical care physician (who is also a methodologist) (see appendix 1 on bmj.com for details of panel members). The panel judged death, non-fatal stroke, major extracranial bleeding, functional ability, and quality of life as critical outcomes. Myocardial infarction, recurrent transient ischaemic attack, and minor extracranial bleeding were judged less important.
The panel requested a systematic review and meta-analysis of RCTs examining the benefits and harms of DAPT versus single agent antiplatelet in order to inform the recommendation. The panel then met online to discuss the evidence and to formulate recommendations. In our judgment no panel member had relevant financial conflicts of interest; intellectual and professional conflicts were minimised and transparently described (see appendix 1 on bmj.com).
The panel followed the BMJ Rapid Recommendations procedures for creating a trustworthy recommendation,2021 including using the GRADE approach to critically appraise the evidence and translate it to recommendations (see appendix 2 on bmj.com).4 The panel considered the benefits, harms and burdens of DAPT versus single antiplatelet therapy, the quality (certainty) of the evidence for each outcome, variations in patient values and preferences, as well as acceptability and feasibility.22 Following the GRADE based approach, recommendations can be strong or weak for or against a specific course of action.23 The recommendations take a patient-centred perspective that de-emphasises public health, societal, and health payer points of view. Healthcare systems can adapt these recommendations by including costs and other key issues of relevance, contextualised to national and local circumstances.
The evidence
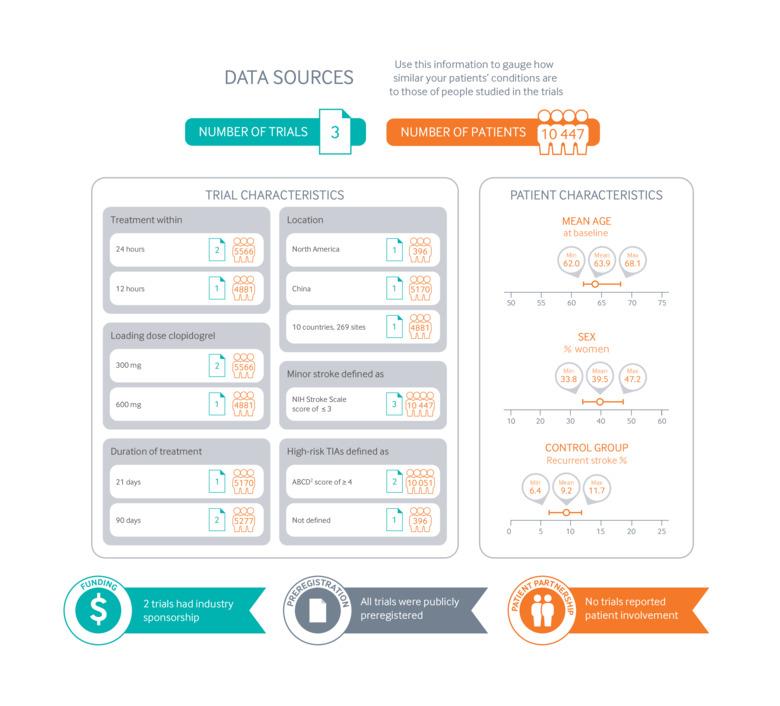
The linked systematic review1 found three RCTs examining DAPT versus aspirin alone reporting on a total of 10 447 patients.21516 Figure 2 provides an overview of the RCTs and RCT participants. Overall, patients included in these trials were similar to those seen in everyday practice. Mean age varied from 62 to 68.1 years. In the FASTER trial 1/6 of the patients were older than 81 years; in CHANCE 1/4 of patients were over 72; and in POINT 1/4 were over 85. Just over half of participants (52.8-66.2%) were male.

Characteristics of patients and trials included in systematic review of the use of DAPT (clopidogrel plus aspirin) versus aspirin monotherapy given within 12-24 hours of symptom onset in patients with high risk transient ischaemic attack (TIA) or minor stroke
{kind=link}
Compared with single antiplatelet therapy,
DAPT decreased all (ischaemic and haemorrhagic) non-fatal recurrent stroke (risk ratio 0.70 (95% confidence interval 0.61 to 0.80), high certainty)
DAPT led to small improvements in functional disability (moderate certainty) and quality of life (moderate certainty)
DAPT led to a small, possibly important increase in moderate or major extracranial bleeding (moderate certainty) (see main infographic).
The RCTs varied from 396 participants to 5170; the two largest trials contributed 10 051 patients. One trial was conducted in China,15 one in North America,16 and one, the POINT trial,2 in 269 study sites from 10 countries worldwide. The POINT trial2 included a diverse population and may therefore be more generalisable than the CHANCE trial, which included only Chinese patients.15 All trials defined minor stroke as a National Institutes of Health Stroke Scale (NIHSS) score of ≤3 at the time of randomisation (scores range from 0 to 42, with higher scores indicating greater deficits). The two large trials defined high risk transient ischaemic attacks as an ABCD2 score of ≥4 (see box 2 for details) at the time of randomisation.17 In all trials, patients had undergone computed tomography (CT) scan or magnetic resonanceimaging (MRI) to exclude the presence of cerebral haemorrhage or alternative explanations for their symptoms. Enrolment had to take place within 12-24 hours of onset of symptoms.
Understanding the recommendation
Absolute benefits and harms
The infographic provides an overview of the recommendation, the benefits and harms, and our certainty in the evidence. Estimates of baseline risk are generated from the control arm of the POINT trial because it was a multinational study and so the population was more diverse.
Overall, the panel was confident that DAPT, when started within 24 hours of symptom onset and used for 10-21 days:
Reduces non-fatal recurrent stroke (ischaemic and haemorrhagic) in the first 90 days by 1.9% (high quality evidence)
Reduces the incidence of moderate or severe functional disability by 1.4% (moderate quality evidence)
Reduces the incidence of poor quality of life by 1.3% (moderate quality evidence).
However, DAPT has little or no impact on:
All-cause mortality (moderate quality evidence)
Incidence of myocardial infarction or recurrent transient ischaemic attack (moderate quality evidence).
Furthermore, DAPT also has some harms:
A small (0.2%), possibly important increase in moderate to major extracranial bleeding events (moderate quality evidence)
A small increase in the risk of minor extracranial bleeding events by 0.7% (high quality evidence).
Patient-important functional disability was defined as modified Rankin scale score of ≥2 as defined by the panel (see table 2).
Definitions of the modified Rankin scale
Duration of DAPT with clopidogrel and aspirin
The panel was confident that DAPT given for 10-21 days compared with 22-90 days results in:
Absolute risk decrease of 0.4% in recurrent ischaemic stroke (moderate quality evidence of no benefit on stroke reduction with prolonged clopidogrel)
Absolute risk decrease of 0.3% in moderate to major bleeding events (high quality evidence).
The maximum benefit occurred in the first 10 days.
Values and preferences
The panel discussed how patients might weigh the benefit of reduced stroke with DAPT against its harm of increased bleeding. The panel believed that most patients would consider a stroke considerably worse than a bleed and so would choose DAPT over single agent therapy. There was no published evidence to support this from patients considering DAPT, but this view is consistent with a systematic review of values and preferences in decision making for antithrombotic therapy.18 In that scenario patients considered non-fatal stroke (thrombotic or haemorrhagic) to be two to three times worse than serious gastrointestinal bleeding.
The panel believed that all or almost all patients would choose 10-21 days of therapy rather than 22-90 days as shorter therapy is associated with equivalent benefit and less harm.
Practical issues
Figure 3 outlines the key practical considerations.

Practical issues about use of DAPT (clopidogrel plus aspirin) versus aspirin monotherapy for patients with high risk transient ischaemic attack or minor stroke
{kind=link}
When should patients begin their DAPT?
If brain imaging is done within 24 hours of onset of symptoms, patients should begin DAPT as soon as the imaging results exclude intracranial haemorrhage or stroke-mimicking lesions. If a delay of 24 hours or more in imaging is suspected, then patients should begin DAPT as soon as a clinician makes a diagnosis of minor ischaemic stroke or transient ischaemic attack, be the clinician a primary care doctor or stroke neurologist, and be the setting inpatient or outpatient. Such patients should have imaging as soon as possible.
How should patients respond if experiencing adverse effects of DAPT?
We are most confident of the stroke reduction with clopidogrel in the first seven days after commencement. If adverse effects are minor, patients may be well advised to continue until at least seven days.
Dosing of antiplatelets
There were no head to head comparisons in the studies to give clear guidance on what loading and maintenance dose to offer. However, the following considerations may be useful:
For clopidogrel—A loading dose of 300 mg and a dose of 75 mg thereafter seem reasonable because bleeding was marginally greater in the POINT trial,2 which used a higher loading dose (table 3)
For aspirin—A dose between 75 mg and 345 mg seems reasonable. The results of the trials do not offer particular insights. Some clinicians may prefer to prescribe at the low end of this range to minimise harm. However, other clinicians may wish to take into account recent evidence of dosing based on weight from studies in primary prevention of cardiovascular events and long term secondary prevention of stroke.19
Clopidogrel and aspirin doses used in intervention arms of the trials included in the systematic review1
The addition of a second agent, likely clopidogrel, adds to the immediate cost of treatment. This drug is, however, widely available and relatively inexpensive, and the duration of use is short. Moreover, the cost savings related to stroke reduction are likely to be as much or more than the costs of clopidogrel administration.
Uncertainties
The following remains uncertain for clinicians and patients:
What is the optimal starting dose of clopidogrel or aspirin? What is the optimal maintenance dose of both agents?
What are the benefits and risks of DAPT with clopidogrel and aspirin in patients with low risk transient ischaemic attack compared with aspirin alone?
What are the risks and benefits of DAPT in patients with moderate strokes (NIHSS score 3-10) with or without thrombolysis treatment?
What are the benefits and risks of DAPT with clopidogrel and aspirin compared with clopidogrel alone in this population?
Updates to this article
Table 4 shows evidence that has emerged since the publication of this article. As new evidence is published, a group will assess the new evidence and make a judgment on to what extent it is expected to alter the recommendation.
New evidence which has emerged after initial publication
Education into practice
For prevention of recurrent stroke in patients with recent transient ischaemic attacks or minor stroke, which antiplatelet or combination of antiplatelets do you prescribe?
How do you identify patients with transient ischaemic attacks as high risk or low risk?
How do you classify stroke as minor or major?
Based on this article, how do you think your personal practice might change? Is there anything that you would do differently for patients with high risk transient ischaemic attack or minor stroke?
How patients were involved in the creation of this article
Three people with lived experience of stroke, and one person with lived experience as a carer for a patient with stroke, were full panel members. They identified and rated outcomes, and led the discussion on values and preferences. The patient partners rated all included outcomes as important to them. Although these values may not be shared by all patients for all outcomes considered, the panel expected little variation in how much importance other patients would place on the critical outcomes of recurrent non-fatal stroke, moderate to major bleeding events, all-cause mortality, functional disability and quality of life.
Patients and carers were instrumental to this guideline in weighing the benefits and harms of DAPT. They clearly articulated the consistent view that avoiding recurrent stroke is paramount in those with transient ischaemic attack and minor stroke and that most would be willing to risk extracranial bleeding to achieve this.
We thank them for their time and valuable input.
Footnotes
This BMJ Rapid Recommendation article is one of a series that provides clinicians with trustworthy recommendations for potentially practice changing evidence. BMJ Rapid Recommendations represent a collaborative effort between the MAGIC group (http://magicproject.org/) and The BMJ. A summary is offered here and the full version including decision aids is on the MAGICapp (https://app.magicapp.org), for all devices in multilayered formats. Those reading and using these recommendations should consider individual patient circumstances, and their values and preferences and may want to use consultation decision aids in MAGICapp in language patients can easily understandto facilitate shared decision making. We encourage adaptation and contextualisation of our recommendations to local or other contexts. Those considering use or adaptation of content may go to MAGICapp to link or extract its content or contact The BMJ for permission to reuse content in this article.
Contributors: All panel members participated in the teleconferences and email discussions and met all authorship criteria.
Competing interests: All authors have completed the BMJ Rapid Recommendations interests disclosure form, and a description of all disclosures is reported in appendix 1 on bmj.com. As with all BMJ Rapid Recommendations, the executive team and The BMJ judged that no panel member had any financial conflict of interest. Professional and academic interests are minimised as much as possible, while maintaining necessary expertise on the panel to make fully informed decisions.
Funding: This guideline was not funded.
Transparency: K Prasad affirms that the manuscript is an honest, accurate, and transparent account of the recommendation being reported; that no important aspects of the recommendation have been omitted; and that any discrepancies from the recommendation as planned (and, if relevant, registered) have been explained.
Provenance and peer review: Commissioned; externally peer reviewed