Screening and management of atrial fibrillation in primary care
BMJ 2021; 373 doi: https://doi.org/10.1136/bmj.n379 (Published 12 April 2021) Cite this as: BMJ 2021;373:n379
- Shiva P Ponamgi, internist, assistant professor1,
- Konstantinos C Siontis, cardiac electrophysiologist, assistant professor2,
- David R Rushlow, family medicine, assistant professor3,
- Jonathan Graff-Radford, neurologist, associate professor4,
- Victor Montori, endocrinologist, professor5 6,
- Peter A Noseworthy, electrophysiologist, professor2 6
- 1Division of Hospital Internal Medicine, Mayo Clinic Health System, Austin, MN, USA
- 2Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA
- 3Department of Family Medicine, Mayo Clinic, Rochester, MN 55905, USA
- 4Department of Neurology, Mayo Clinic, Rochester, MN, USA
- 5Division of Endocrinology, Mayo Clinic, Rochester, MN, USA
- 6Knowledge and Evaluation Research Unit, Mayo Clinic, Rochester, MN, USA
- Correspondence to: P A Noseworthy noseworthy.peter{at}mayo.edu
Abstract
Atrial fibrillation is a common chronic disease seen in primary care offices, emergency departments, inpatient hospital services, and many subspecialty practices. Atrial fibrillation care is complicated and multifaceted, and, at various points, clinicians may see it as a consequence and cause of multi-morbidity, as a silent driver of stroke risk, as a bellwether of an acute medical illness, or as a primary rhythm disturbance that requires targeted treatment. Primary care physicians in particular must navigate these priorities, perspectives, and resources to meet the needs of individual patients. This includes judicious use of diagnostic testing, thoughtful use of novel therapeutic agents and procedures, and providing access to subspecialty expertise. This review explores the epidemiology, screening, and risk assessment of atrial fibrillation, as well as management of its symptoms (rate and various rhythm control options) and stroke risk (anticoagulation and other treatments), and offers a model for the integration of the components of atrial fibrillation care.
Introduction
Atrial fibrillation, a chaotic heart rhythm characterized by an irregular and often rapid heart rate, is a common arrhythmia.1 Its incidence and public health impact are growing as a result of the increasing multi-morbidity and longevity of the population and increasing ease of diagnosis.2345 Despite increasing availability of methods for diagnosis, much of atrial fibrillation goes undetected and under-diagnosed.67
Although some patients with atrial fibrillation have no symptoms,78 many experience bothersome palpitations, shortness of breath, or exercise intolerance. A subset develop complications including thromboembolism/stroke,9101112 heart failure,13 or cognitive impairment,14 and atrial fibrillation is associated with a nearly twofold excess risk of all cause mortality.15 Prevalence of atrial fibrillation increases with age, and it commonly coexists with other comorbidities that are typically cared for in a primary care setting, such as hypertension, sleep apnea, and obesity.
No definitive cure for atrial fibrillation exists, so its management focuses on four main pillars: efforts to correct risk factors, lifestyle interventions, and comorbidities; rate control strategies; rhythm control strategies; and reduction of stroke risk (fig 1). Specific therapies can range from simple medications to invasive procedures, including catheter ablation, pacemaker implantation, left atrial appendage occlusion, and even cardiac surgery. Navigating this wide array of options in a complex and diverse population requires active patient engagement in decision making and careful consideration of context and preferences. Herein, we review the current state of screening, diagnosis, risk stratification, and management for atrial fibrillation.
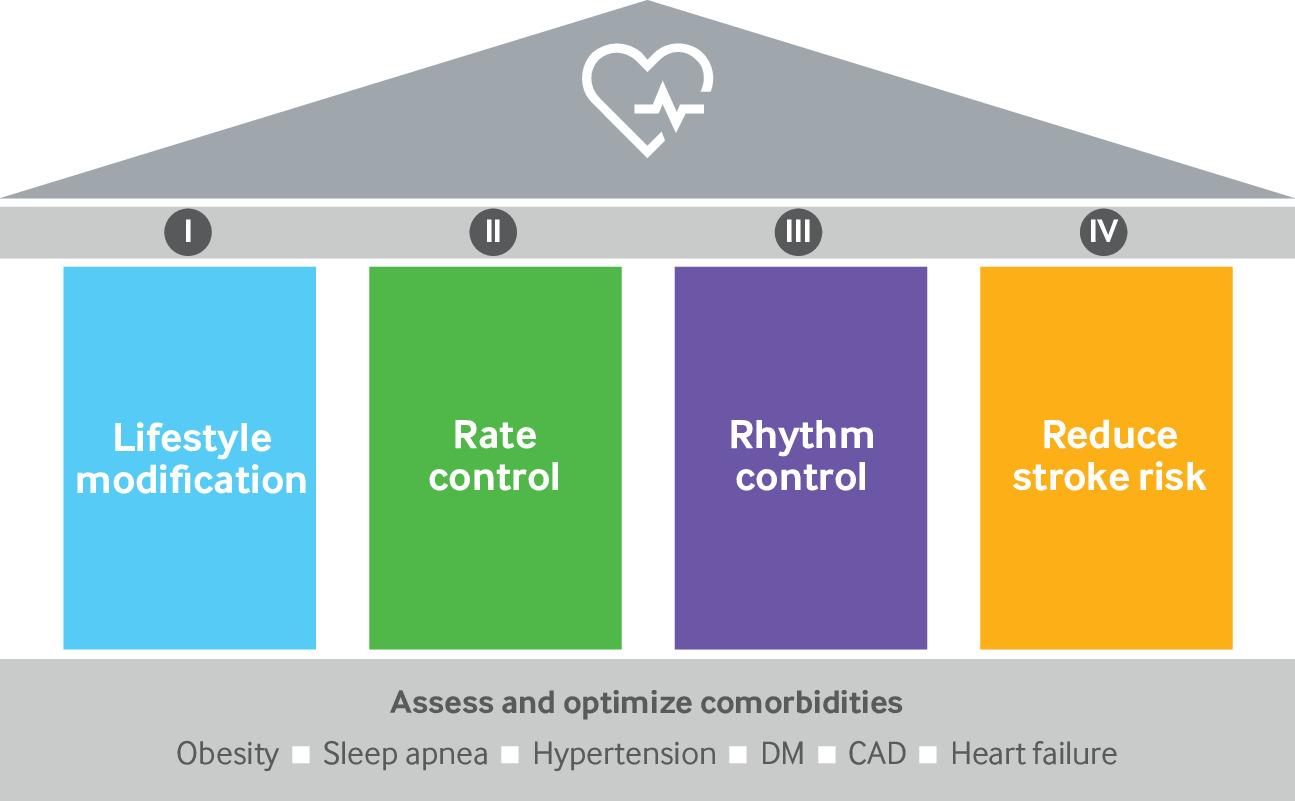
Pillars of atrial fibrillation management as described in American Heart Association scientific statement outlining lifestyle and risk factor modification for reduction of atrial fibrillation.16 CAD=coronary artery disease; DM=diabetes mellitus
{kind=link}
Sources and selection criteria
We identified literature through a search of PubMed until January 2020 for keywords including “atrial fibrillation AND epidemiology” OR “atrial fibrillation AND natural history” OR “atrial fibrillation AND stroke risk” OR “CHA2DS2-VASc” OR “CHADS2” OR “HAS-BLED” OR “atrial fibrillation AND warfarin” OR “atrial fibrillation AND direct oral anticoagulants” OR “atrial fibrillation AND novel oral anticoagulants” OR “atrial fibrillation AND apixaban” OR “atrial fibrillation AND dabigatran” OR “atrial fibrillation AND rivaroxaban” OR “atrial fibrillation AND edoxaban” OR “atrial fibrillation AND screening” OR “atrial fibrillation AND treatment”. Owing to the vast number of studies in the search results (68 824 results), we prioritized studies that were randomized controlled trials (RCTs), systematic reviews, or meta-analyses to gather the strongest level of evidence for each topic being discussed (5396 results) and then limited the results to studies in humans that were published in English in the past 10 years (3148 results). We also included relevant observational studies that were published in journals that are clinically focused and have a high impact factor to present a comprehensive outlook. We reviewed abstracts of all the studies to categorize the relevant ones for inclusion and discarded studies irrelevant to our topic. We also searched the references of included studies for further relevant studies. We prioritized recent studies with larger sample sizes over older and smaller studies. We included older studies only if important and pertinent to the topic being discussed or if recent research in that area was unavailable.
Epidemiology
Atrial fibrillation is estimated to affect more than 30 million people globally.1 The incidence and prevalence of atrial fibrillation have increased steadily over the past 20 years, and it will doubtless present a growing public health challenge.2 The increased prevalence of atrial fibrillation may be due to increasing multi-morbidity and longevity, as well as the widespread availability of more sensitive rhythm monitoring methods that allow earlier detection of arrhythmia.345 Furthermore, this apparent increase in prevalence may be an underestimate, as much of atrial fibrillation is asymptomatic and undiagnosed.6 In a community based cohort with manually validated new diagnoses of atrial fibrillation, one in three patients had no symptoms whatsoever at the time of coincidental detection of atrial fibrillation by electrocardiography performed for a different reason.7
Several non-modifiable and modifiable risk factors are recognized as playing a role in atrial fibrillation. The incidence and prevalence of atrial fibrillation increases with age and is higher in men than in women.17181920 Although the overall prevalence of atrial fibrillation in men is double that in women, among older adults more women than men have atrial fibrillation owing to the longer longevity of women.21 A familial predisposition to atrial fibrillation is also recognized, but in most cases atrial fibrillation is not a monogenetic disorder.
Structural, functional, and electrophysiological changes resulting from a complex interplay of risk factors are thought to be responsible for the initiation, progression, and maintenance of atrial fibrillation.22 In many patients, these changes may include left ventricular hypertrophy, diastolic dysfunction, left atrial enlargement, left atrial fibrosis, left atrial stiffness, and autonomic dysfunction. In other cases of atrial fibrillation especially in young patients, no identifiable risk factors may exist, suggesting a possible genetic predisposition.232425 Regardless, atrial fibrillation can by itself sustain and further promote atrial, ventricular, and systemic structural and functional alterations. Thus, breaking this vicious cycle requires targeting of both the risk factors for atrial fibrillation and the atrial fibrillation itself.
Natural history of atrial fibrillation
The natural history of atrial fibrillation is highly variable but tends to follow a progression from a paroxysmal pattern to a more persistent and even chronic pattern over time. However, as much of atrial fibrillation may result in no symptoms, the natural history of subclinical atrial fibrillation and the true burden of the arrhythmia are poorly characterized.262728 In experimental animal models, the observation that structural and electrophysiological substrate changes worsen as a function of the chronicity of the arrhythmia (“atrial fibrillation begets atrial fibrillation”) has led to the prevailing hypothesis that atrial fibrillation progresses to an increasingly permanent form over time.293031 Atrial fibrillation is classified as “paroxysmal” if episodes terminate spontaneously or after targeted intervention within seven days, whereas atrial fibrillation lasting more than seven days without termination is considered “persistent” and often requires electrical or pharmacological cardioversion for termination. Atrial fibrillation that persists continuously for longer than a year is termed “longstanding persistent atrial fibrillation.” Finally, when the patient and clinician decide not to pursue any attempt to restore normal rhythm, atrial fibrillation is considered “permanent.” The rapidity of progression from a paroxysmal to more persistent or permanent arrhythmia varies and is affected by the control of comorbid/underlying conditions, as well as other, as yet unidentified factors. Some evidence is increasingly suggesting that early treatment may improve clinical outcomes.3233
Atrial fibrillation is so common in older populations that it can seem to be an inevitable consequence of aging. However, more than 50% of the incidence of atrial fibrillation in some populations is thought to be the result of suboptimal risk factor control.34 Like many chronic conditions, atrial fibrillation is highly related to common comorbidities, and lifestyle interventions are the backbone of preventive care (fig 2). Although some risk factors for atrial fibrillation are not modifiable (age,1718 male sex,1920 or family history, for instance), patients should be aware that they can reduce the risk and burden of atrial fibrillation through lifestyle interventions.3637 The Framingham Heart Study identified hypertension, congestive heart failure, coronary artery disease, and diabetes mellitus as risk factors for the development of atrial fibrillation.20 Obesity, obstructive sleep apnea, and other lifestyle factors such as chronic endurance training have also been associated with increased risk of atrial fibrillation.383940 Comorbidities such as hypertension, valvular heart disease, chronic obstructive pulmonary disease, and cerebrovascular disease are known to predict progression of atrial fibrillation and poor response to catheter ablation.4142 These risk factors should also be considered as targets for prevention of atrial fibrillation in the primary care setting (fig 2).
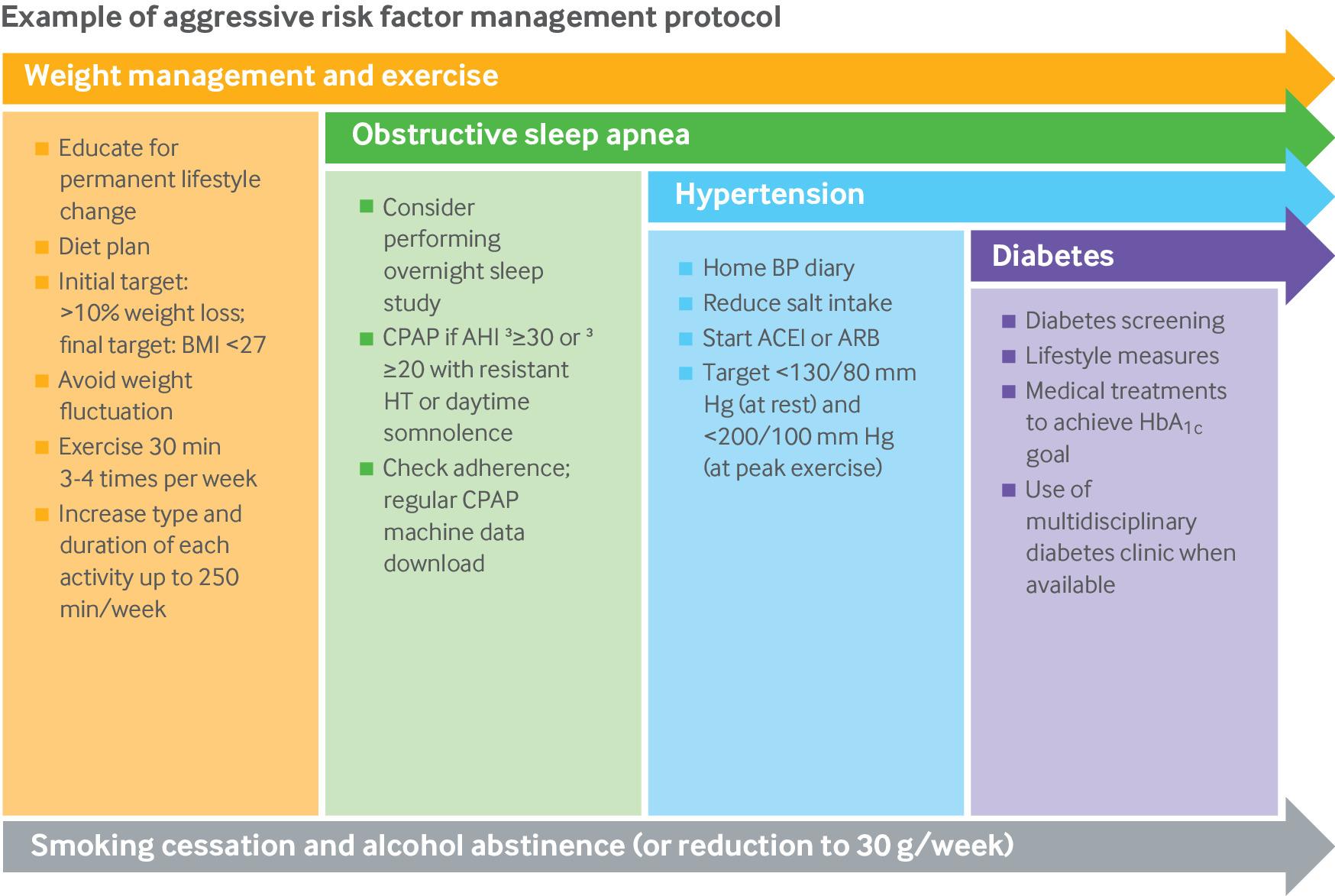
Components of risk factor modification in primary and secondary prevention of atrial fibrillation. ACEI=angiotensin converting enzyme inhibitor; AHI=apnea-hypopnea index; ARB=angiotensin II receptor blocker; BMI=body mass index; BP=blood pressure; CPAP=continuous positive airway pressure; HbA1c=hemoglobin A1c; HT=hypertension. Adapted from Lau et al35
{kind=link}
Screening for atrial fibrillation
Screening for indolent or asymptomatic diseases that are common but treatable is central to the mission of primary care. To be valuable, a screening test must have sufficient precision, and effective and safe downstream interventions that can improve outcomes must exist. Whether screening for atrial fibrillation fulfils these criteria is controversial, however, and current guidelines and many professional societies do not recommend routine screening in primary care. For instance, the 2019 UK National Screening Committee posed a series of criteria that would need to be established to justify screening and then, after performing an exhaustive evidence review around each criterion, concluded that many factors remain “uncertain” so that screening is not recommended at this time.43 The criteria they explored included the relative risk of stroke based on type of atrial fibrillation, evidence for a benefit of treating atrial fibrillation detected by screening, the reported accuracy of screening tests for atrial fibrillation, the availability of RCT level evidence of a benefit of screening, cost effectiveness, and clinical infrastructure of optimal treatment. Similarly, the United States Preventive Services Task Force has concluded that the current evidence is insufficient to assess the balance of benefits and harms of screening for atrial fibrillation with electrocardiography,44 and the 2014 National Institute for Health and Care Excellence atrial fibrillation guidelines refer to pulse palpation as the only recommended screening assessment for atrial fibrillation, but only in patients with symptoms.45
Why then does this remain controversial? Data are certainly mixed, and the role for targeted screening of patients at risk may evolve over time as rhythm monitoring technologies are further refined and as the evidence base is further developed.464748 Among patients with a cryptogenic stroke who undergo 30 day rhythm monitoring, as many as about 15% are found to have previously undiagnosed paroxysmal atrial fibrillation.49 The observational STROKESTOP study in Sweden showed that population based electrocardiographic screening of people aged 75 years or older was associated with a reduction in the occurrence of ischemic strokes at five years of follow-up.50 In the area where screening for atrial fibrillation was implemented, ischemic stroke declined from 14.5 to 9.1 per 1000 person years (P=0.003), whereas the incidence did not change significantly in the control area (from 12.7 to 11.2 per 1000 person years; P=0.31).
A desire to prevent strokes, coupled with the exponential growth of mobile and wearable rhythm monitoring technologies, has led to a heightened interest in the role of screening general populations for atrial fibrillation.51 Possible low cost and convenient screening methods include pulse palpation,52 automated blood pressure monitors, single lead or multi-lead electrocardiography devices,535455 insertable monitors,5657 and even pulse photoplethysmography58 or electrocardiography based smartwatch applications. Most notably, in the recent Apple Heart Study, the largest pragmatic evaluation of atrial fibrillation screening in a general population using a smartwatch enabled pulse photoplethysmography technology, 0.52% of participants received notifications of possible atrial fibrillation over an average of more than three months of monitoring.59 In about a third of these people, atrial fibrillation was later confirmed by week long patch electrocardiography monitoring. This suggests that although mass screening of unselected populations is feasible with current technologies, the yield of such an approach is low, and the clinical impact is uncertain. One should also weigh in the drawbacks of monitoring and diagnosis related anxiety, as well as the unclear indications for treatment of atrial fibrillation detected by long term rhythm monitoring. For example, the effect of the duration and burden of atrial fibrillation on treatment decisions is largely unknown, and further population based studies are needed to evaluate the value of smartwatches in long term screening for atrial fibrillation.58
More than a dozen ongoing prospective studies are examining the role of screening for atrial fibrillation, and this growing body of evidence will certainly inform future recommendations.60 For now, however, we acknowledge that although screening can detect asymptomatic atrial fibrillation, the downstream benefit of widespread implementation of screening in unselected populations is unproven.61
Risk assessments
CHA2DS2-VASc
Identifying patients with atrial fibrillation who are at sufficient risk of cardioembolic stroke to warrant systemic anticoagulation is a clinical and research priority. Nearly 20 years ago, before the introduction of direct oral anticoagulants (DOACs), the CHADS2 scoring system was developed and validated.12 The system scores 1 point each for recent exacerbation of congestive heart failure, history of hypertension, age 75 years or older, and type 2 diabetes mellitus and 2 points for history of previous transient ischemic attack or stroke. Although this scoring system was rapidly adopted in practice, the overall performance is modest with an area under the curve typically in the 0.65-0.7 range. The scoring system also does not account for potentially powerful risk factors such as sex and underlying vascular disease, and it classifies a large proportion of patients in an intermediate risk category.62
The risk stratification scheme was subsequently refined as the CHA2DS2-VASc score,63 which includes three additional factors: female sex, age 65-74 years, and vascular disease. The CHA2DS2-VASc score delineates the following risk categories for thromboembolism and recommended treatment approaches based on the 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society (AHA/ACC/HRS) atrial fibrillation guideline64: 0=low risk (annual risk 0.3%; anticoagulation generally not recommended), 1=low-moderate risk (annual risk 0.9%; consider anticoagulant), and ≥2=moderate-high risk (annual risk >2.9%; anticoagulation recommended). The most valuable aspect of this newer scoring system is that it can identify people in the lowest risk category (score=0) as having a very low risk of stroke, and clinicians can be more confident in not offering anticoagulation for this group. However, the proportion of patients falling into this category is small (<10%) and as many as 80% of the total atrial fibrillation population are categorized as at least intermediate risk (score of 2 or higher),65 resulting in a recommendation to anticoagulate a large majority of atrial fibrillation patients on the basis of the 2014 AHA/ACC/HRS atrial fibrillation guideline.64 An analysis suggested that this guideline’s recommendation for use of the CHA2DS2-VASc and corresponding treatment thresholds resulted in an increase in the overall proportion of atrial fibrillation patients recommended for oral anticoagulation from 71.8% to 90.8% in the US.66 This corresponds to an increase in the number of patients recommended for anticoagulation from an estimated 3.7 million to 4.7 million. Furthermore, the overall discriminating performance of this scoring system is only marginally improved over the CHADS2 score, with areas under the curve typically estimated in the 0.68-0.7 range. The overall modest performance of these scoring systems, as well as the fact that they result in a recommendation to anticoagulate most patients (many of whom do not go on to have a stroke), particularly given the cost of the newer agents, has led many people to call for newer risk stratifications schemes, developed without influence of industry partners who could benefit from broad indications for anticoagulation.
HAS-BLED
Patients treated with anticoagulants are at increased risk of bleeding on treatment, which has also prompted the development of scoring systems to quantify bleeding risk. Although many such scoring systems have been developed, the HAS-BLED score has gained popularity and widespread adoption owing to its ease of use and accuracy in predicting bleeding risk in patients on anticoagulation.67686970 The HAS-BLED compiles risk factors including hypertension, renal disease, liver disease, stroke history, previous bleeding or predisposition to bleeding, labile international normalized ratio (INR), age above 65 years, medications predisposing to bleeding, and alcohol use (1 point each). The score can be used in patients not taking a vitamin K antagonist (VKA), but the variable for a labile INR is omitted from the calculation.68 According to the HAS‐BLED score, atrial fibrillation patients are subdivided into three risk categories, in which a score of 0 indicates low risk, 1-2 indicates moderate risk, and 3 or higher indicates high risk. Various validation studies have examined HAS-BLED in predicting bleeding risk while on anticoagulation (both VKA and non-VKA anticoagulants), taking aspirin, or without any antithrombotic therapy. HAS-BLED is also the only score shown to be predictive of intracranial hemorrhage. The HAS-BLED score has also been validated in non-atrial fibrillation populations, including those with venous thromboembolism,71 acute coronary syndrome, or percutaneous coronary interventions and those undergoing anticoagulant bridging therapy.72
Clinical application of risk assessments
Current guidelines recommend the CHA2DS2-VASc scoring system,6373 which aggregates common risk factors to estimate a patient’s risk and guide treatment decisions. This risk stratification approach does not apply to atrial fibrillation patients with severe mitral stenosis, mechanical valve prostheses, known atrial thrombus, hypertrophic or amyloid cardiomyopathy, or congenital heart disease. In these situations, anticoagulation is generally recommended in all patients with atrial fibrillation.
Clinicians and patients must frame decisions about anticoagulation in terms of how it will affect daily routines, hobbies, and work; how much it will cost and what demands it will make it on the patient’s time; and the potential bleeding risk. Although the HAS-BLED score is the most widely accepted system to estimate bleeding risk,67686970 a high HAS-BLED score by itself is not a reason to withhold anticoagulation as risks for bleeding and stroke usually correlate. Patients with a high HAS-BLED score include those who may derive even greater net clinical benefit from anticoagulation owing to its effect on reduction of stroke risk. Instead of identifying patients who should not be anticoagulated, the HAS-BLED score should be used to flag those potentially at risk of bleeding who may warrant particularly careful monitoring and follow-up. Also, HAS-BLED draws attention to well established potentially reversible risk factors for bleeding, such as uncontrolled hypertension, labile INR, concomitant use of aspirin/non-steroidal anti-inflammatory drugs, or alcohol excess.
The HAS-BLED score may underestimate bleeding risk in a subset of atrial fibrillation patients. Several conditions present a challenge in decision making, including chronic subdural hematoma, cerebral vascular malformations, gastrointestinal conditions that predispose to bleeding and may be difficult to treat (Crohn’s disease, angiodysplasia), and hematological disorders of coagulation. Cerebral amyloid angiopathy (CAA), which involves β-amyloid deposition in cerebral blood vessels, is especially relevant in older people with atrial fibrillation and is a common cause of anticoagulant related intracranial hemorrhage.74 One meta-analysis estimated a 7.4% annual risk of CAA related recurrent intracranial hemorrhage, comparable in many older atrial fibrillation patients to the risk of ischemic stroke if untreated.75
Clinically, CAA most often manifests with lobar hemorrhage but can also be detected in patients without symptoms with hemosiderin sensitive magnetic resonance imaging (MRI) sequences. As the HAS-BLED score does not account for such asymptomatic MRI lesions, the score may underestimate bleeding risk in this population.76 Both CAA and atrial fibrillation increase significantly with age, and people may undergo brain MRIs for a variety of indications; therefore, clinicians are more commonly encountering patients with both atrial fibrillation and CAA, resulting in clinical management dilemmas. Patients with CAA and atrial fibrillation have an indication for anticoagulation to reduce ischemic stroke risk and an elevated risk of intracranial hemorrhage. An individualized approach with a multidisciplinary team is recommended in these patients, taking into account the patient’s preference, the patient’s risk of ischemic stroke (CHA2DS2Vasc), the burden of CAA detected on MRI, and medical comorbidities. No prospective trials of treatment approaches in this patient population have been conducted, but warfarin should generally be avoided in favor of DOACs or left atrial appendage closure if the ischemic stroke risk justifies treatment.77
Oral anticoagulation
Why and when should we treat with warfarin, and should DOACs be first line?
Oral anticoagulation options in the care of atrial fibrillation patients have expanded in the past 10 years beyond the well established VKAs, such as warfarin, which are limited by drug-drug and drug-food interactions, the need for frequent blood tests/INR testing, and notoriously variable time in therapeutic range.787980 The availability of the DOACs in clinical practice (dabigatran, rivaroxaban, apixaban, and edoxaban) has dramatically changed the landscape of anticoagulation. They are increasingly preferred over VKAs in eligible patients owing to their ease of use, avoidance of frequent blood draws for therapeutic monitoring, lower risk of intracranial bleeding, and decreased concerns about drug and food interactions. Also, DOACs have a rapid onset of action and short half-life and attain more predictable blood concentrations, allowing standard fixed dosing regimens and obviating the need for laboratory monitoring (table 1). These factors, along with lower risk of major bleeding including intracranial hemorrhage, provide considerable advantages of DOACs over warfarin for thromboembolic prophylaxis in patients with atrial fibrillation.64818283
Comparison of direct oral anticoagulants and warfarin
Since the introduction of DOACs, an increase has been reported in the use of guideline recommended therapy in patients newly diagnosed as having atrial fibrillation and at risk of stroke.8485 In patients with acute ischemic stroke and atrial fibrillation, DOAC use at discharge was associated with better long term outcomes relative to warfarin.86 In the seminal randomized trials, DOACs have been shown to be as effective as or more effective than warfarin in preventing stroke irrespective of the patients’ comorbidities, as they conferred similar or lower rates of both ischemic stroke and major bleeding, as shown in several randomized trials.878889909192 In a meta-analysis of 13 RCTs in patients with venous thromboembolism or atrial fibrillation, DOACs were associated with a significantly lower risk of major bleeding (relative risk 0.72, 95% confidence interval 0.62 to 0.85; P<0.01; I2=78%), fatal bleeding (0.53, 0.43 to 0.64; P<0.01; I2=0%), intracranial hemorrhage (0.43, 0.37 to 0.50; P<0.01; I2=2%), clinically relevant non-major bleeding (0.78, 0.68 to 0.90; P<0.01; I2=89%), and total bleeding (0.76, 0.71 to 0.82; P<0.01; I2=86%). No significant difference was seen in major gastrointestinal bleeding between DOACs and VKAs (relative risk 0.94, 0.75 to 1.99; P=0.62, I2=71%).93 Another meta-analysis that included data from four RCTs in patients with atrial fibrillation concluded that DOACs have a favorable risk-benefit profile compared with warfarin, with significant reductions in stroke (relative risk 0.81, 0.73 to 0.91; P<0.001), intracranial hemorrhage (0.48, 0.39 to 0.59; P<0.0001), and mortality (0.90, 0.85 to 0.95; P<0.001). The risk of major bleeding was similar to that with warfarin, but the risk of gastrointestinal bleeding was greater with DOACs (relative risk 1.25, 1.01 to 1.55; P=0.04).94 Other studies have also shown a reduction in fatal bleeding with DOACs compared with VKAs.959697
Although DOACs have a safer bleeding profile than warfarin, major bleeding still occurs in about 3-4% of patients taking DOACs every year.98 Despite a lower incidence than warfarin, intracranial hemorrhage associated with DOAC usage remains a concern. Intracranial hemorrhage is responsible for up to 45% of all bleeding related deaths in DOAC treated patients and carries a fourfold increased risk of mortality compared with major extracranial bleeds.99 One of the key concerns with the initial DOAC experience was the lack of reversal agents. The recent availability of reversal agents for DOACs is anticipated to further increase the comfort level of clinicians and patients using these agents.100101 However, feedback from our patient reviewers suggests that the greater familiarity and experience with warfarin reversal remains a major advantage of warfarin over DOACs from their perspective. Clinicians should also be aware that DOACs remain expensive and may not be affordable for many patients across different healthcare systems and medication reimbursement programs.
Finally, DOACs are contraindicated in patients with mechanical valve prostheses owing to an increased risk of thrombosis.102 Even though very few patients with severe native valve disease and bioprosthetic valve prostheses were included in the DOAC trials, subsequent analyses have shown that DOACs are reasonable choices in these patients, except for those with severe rheumatic mitral stenosis.103 Although the initial trials of these agents excluded patients with end stage renal disease on dialysis, the use of apixaban in clinical practice has shown reasonable safety and effectiveness in this patient population104; however, this is not the case for dabigatran and rivaroxaban.105 Emerging data also suggest that the DOACs are safe and effective in patients with atrial fibrillation and hypertrophic cardiomyopathy.106
Reasons to withhold or stop anticoagulation
Generally, most patients with atrial fibrillation should be treated with anticoagulation. Making the distinction between relative and absolute contraindications for anticoagulation can be challenging and controversial.107108109110111 Absolute contraindications to the use of anticoagulation therapy may include severe thrombocytopenia, recent trauma or surgery, recent hemorrhagic stroke, recent intracranial hemorrhage, intracranial masses, or decompensated liver disease.10112113 Clinicians need to carefully assess each of these risks and weigh the risk of a life threatening bleed against the risk of disabling stroke when withholding anticoagulation.
Although not without controversy, percutaneous left atrial appendage occlusion with a Watchman device (Boston Scientific, St Paul, MN) is an alternate non-pharmacologic method of reducing embolic strokes in atrial fibrillation patients at high risk and with contraindications to long term anticoagulation.114115 The premise of this approach is that most (>90%) thrombi related to atrial fibrillation are formed in the left atrial appendage. The landmark PROTECT-AF trial showed that left atrial appendage occlusion was non-inferior to warfarin for preventing the combined outcome of stroke, systemic embolism, and cardiovascular death (hazard ratio 0.40, 95% confidence interval 0.21 to 0.75; P=0.005) and all cause mortality (0.66, 0.45 to 0.98; P=0.04).116 Subsequent randomized clinical trials, including the PREVAIL and the ASAP studies, as well as patient level meta-analyses reaffirmed the non-inferiority of left atrial appendage occlusion over warfarin in various clinical scenarios and regimens,117118119 but much of the benefit seems to be related to averted intracranial bleeds, rather the prevention of cardioembolic stroke.
Ongoing studies will evaluate the device in patients with absolute contraindications to anticoagulation or in comparison with the DOACs, which may have a more favorable bleeding profile in some patients. In addition to the now well established Watchman device, many other left atrial appendage occlusion devices are being evaluated in clinical trials and are expected to receive approval for routine clinical use soon. Surgical and minimally invasive thoracoscopic options for the exclusion of the left atrial appendage are also available.
Underuse of anticoagulants
The underuse of anticoagulation is an ongoing problem. In one study, fewer than half of eligible patients with a new diagnosis of atrial fibrillation were started on oral anticogulants.120 Underuse of oral anticoagulation has also been shown to be highly prevalent among atrial fibrillation patients admitted with a stroke.121 Despite the availability of convenient options for oral anticoagulation with the DOACs, its use has increased only modestly in recent years.122 Importantly, discontinuation of anticoagulation seems to be most common in patients at high risk of stroke, including older adults and women.
The reasons for such underuse of oral anticoagulation likely include healthcare, provider, and patient related factors. For example, the perceived balance of stroke versus bleeding risk and the priorities in care may be different from the perspective of the primary care provider who focuses on a simplified care model that minimizes polypharmacy compared with the neurologist who cares for patients with debilitating strokes. Patients’ perspectives on oral anticoagulation, knowledge gaps, and even financial constraints likely also affect the rates of use. Educational interventions alone may not always translate to improvement of clinical outcomes. These interventions are most likely to be successful when they involve all pertinent stakeholders, including the patient’s primary and specialty care clinicians and, most critically, the patients themselves.123124
Role of rhythm control
For the patient presenting to the primary care clinic with a new diagnosis of atrial fibrillation, the first decision point hinges on whether to pursue a rhythm control or a rate control strategy (fig 3). Patients with ongoing atrial fibrillation at the time of initial evaluation, as confirmed by 12 lead electrocardiography, and with very slow or rapid ventricular rates (typically <40 bpm and >150 bpm), evidence of hemodynamic instability, severe symptoms, or decompensated heart failure should be referred to the emergency department for stabilization and possible electrical cardioversion. In case of unknown duration of atrial fibrillation, cardioversion should be preceded by transesophageal echocardiography to rule out intracardiac thrombus. Patients are required to be on anticoagulation for at least four weeks after electrical cardioversion to reduce the risk of thromboembolism.

Algorithm for management of initial and breakthrough atrial fibrillation (AF) episodes. AAD=antiarrhythmic drug; BB=β blocker; CCA=calcium channel antagonist; CHF=congestive heart failure; LAA=left atrial appendage; TEE=transesophageal echocardiography
{kind=link}
Although the choice between rate and rhythm control has generally been considered not to have an effect on hard clinical outcomes, such as survival,125126 rhythm control should be favored in the presence of significant atrial fibrillation related symptoms or presumed tachycardia induced cardiomyopathy.127 A rhythm control approach may also be preferable in younger (<65 years) patients with paroxysmal atrial fibrillation, as rate control alone is likely to result in progression to longstanding persistent atrial fibrillation over a period of time, which will later be more difficult to control and carries a risk of development of tachycardia induced cardiomyopathy.128 Young patients may be particularly prone to side effects from rate controlling agents, including fatigue, erectile dysfunction, or depression.129130
If an early rhythm control strategy is chosen, an elective electrical or pharmacologic cardioversion may be performed shortly after diagnosis of atrial fibrillation. We acknowledge, however, that in some cases—for instance, if atrial fibrillation is incidentally detected in a patient with severe comorbidities—an initial rate control strategy may be reasonable. For subsequent episodes, the decision to pursue rate or rhythm control depends on the factors discussed above. The recently completed EAST-AFNET 4 trial provides contemporary evidence in support of an early rhythm control approach.131 It randomized nearly 2800 patients to rhythm or rate control early after their initial diagnosis of atrial fibrillation (median time from diagnosis 36 days). Patients in the rhythm control group had a significantly lower incidence of a composite clinical endpoint, including cardiovascular death, stroke, or hospital admission for heart failure or acute coronary syndrome, compared with the rate control group (3.9 v 5.0 per 100 person years; hazard ratio 0.79, 95% confidence interval 0.66 to 0.94; P=0.005).
Rhythm control: antiarrhythmic drugs
Several antiarrhythmic drugs have been widely used for the past several decades as first line or second line approaches and often adjunctively with an ablation approach. Flecainide and propafenone (class Ic antiarrhythmics132) are typically used in paroxysmal atrial fibrillation and can be used as a pill-in-pocket approach or as scheduled medications. These can typically be initiated in an outpatient setting. Class Ic drugs can have a proarrhythmic effect in the presence of structural heart disease,133 mainly myocardial scar, so their use is reserved for patients with structurally normal hearts. Class III antiarrhythmics such as sotalol and dofetilide can be used in both paroxysmal and persistent atrial fibrillation.134135 Their antiarrhythmic action is related to their effect on prolongation of myocardial repolarization. They have an expected effect on prolongation of the QTc interval, but when this effect is exaggerated they can provoke potentially fatal ventricular arrhythmias (such as torsades de pointes). Therefore, initiation of these drugs warrants admission to hospital for continuous rhythm monitoring and serial electrocardiograms for QTc interval monitoring for the first five or six doses. This practice may vary between different healthcare systems.
Amiodarone is the most effective antiarrhythmic,136 but owing to its toxicity profile it is reserved as a last resort option in patients who have not responded to or not tolerated other antiarrhythmic drugs or catheter ablation.137 The risk of cardiac, pulmonary, thyroid, liver, and ocular toxicities, among other toxicities, is time and dose dependent. Therefore, amiodarone should be avoided in younger patients. When necessary, it is prescribed at the lowest necessary dose, for the shortest time possible, and under close monitoring as discussed later in this review. Dronedarone is structurally and mechanistically similar to amiodarone but lacks the side effect profile of amiodarone. However, its lower effectiveness and other safety concerns have made it a less popular option in the current armamentarium for atrial fibrillation.
The choice of a specific anti-arrhythmic drug is tailored to the individual patient on the basis of their atrial fibrillation phenotype, goals of therapy, and cardiac and non-cardiac comorbidities. Given the complexities described above, shared decision making and guidance on the prescription of antiarrhythmic drugs should involve specialists and primary care physicians.
Rhythm control: role of catheter based interventions
The discovery of ectopic beats from the pulmonary veins triggering paroxysmal atrial fibrillation in humans led to the development of catheter based pulmonary vein isolation as an interventional strategy for the treatment of atrial fibrillation.138139 The 2014 AHA/ACC/HRS guideline for the treatment of atrial fibrillation places ablation as a class I option for the treatment of symptomatic drug refractory persistent atrial fibrillation, but ablation of paroxysmal atrial fibrillation before drug failure is a class IIa recommendation.64 The procedure is directed toward electrically isolating the atrial fibrillation triggers in the pulmonary veins along with supplementary modification of the atrial fibrillation substrate to prevent recurrence of atrial fibrillation and improve the outcomes of the procedure.140
Many studies have evaluated adjuvant ablation strategies to improve rhythm control outcomes in persistent atrial fibrillation, but results are mixed with some studies showing no additional benefit and other showing only marginal gains.141142 Ablation can be performed with thermal tissue injury with radiofrequency energy or tissue freezing with a cryoballoon,143144145 with similar success rates and safety profile.146147148149 Novel approaches including renal denervation through ablation of the renal sympathetic efferent and afferent nerves have been evaluated as a treatment for resistant hypertension and improving the success of atrial fibrillation ablation.150151152
Catheter ablation is effective in reducing the burden of both paroxysmal and persistent atrial fibrillation In the largest catheter ablation trial to date, the CABANA trial, which randomized 2204 patients with atrial fibrillation to catheter ablation or drug therapy, catheter ablation reduced recurrences of atrial fibrillation by 48% compared with antiarrhythmic drug therapy over five years of follow-up. In the trial, the patients in the catheter ablation group experienced significant reduction in both first recurrence of any symptomatic or asymptomatic atrial fibrillation (hazard ratio 0.52, 0.45 to 0.60; P<0.001) or first symptomatic-only atrial fibrillation (0.49, 0.39 to 0.61; P<0.001) at five years of follow-up.153 In the recent CIRCA-DOSE trial—in which 346 patients with drug refractory paroxysmal atrial fibrillation were randomized to contact force guided radiofrequency ablation (n=115), four minute cryoballoon ablation (n=115), or two minute cryoballoon ablation (n=116)—catheter ablation with radiofrequency or cryoballoon resulted in freedom from atrial tachyarrhythmias in slightly more than half of patients, without a difference between ablation approaches (53.9%, 52.2%, and 51.7% with force guided radiofrequency ablation, four minute cryoballoon ablation, and two minute cryoballoon ablation, respectively; P=0.87).154 That reduced atrial fibrillation burden may translate to a lower risk of stroke and other hard outcomes for patients may seem intuitive, but the CABANA and other atrial fibrillation ablation trials have shown no clear reductions in endpoints such as stroke, death, cardiac arrest, or major bleeding with ablation compared with medical therapy.155156 However, the role for early rhythm control remains controversial. In contrast to CABANA, the EAST trial, discussed earlier in this review, showed a reduction in a composite of cardiovascular death, stroke, or hospital admission for heart failure or acute coronary syndrome with early rhythm control.131 However, less than 10% of patients in this study underwent ablation as the initial rhythm control strategy. Although dedicated ablation trials such as RAAFT-1, RAAFT-2, and MANTRA-PAF have not, to date, shown such benefits with ablation alone,157158159 they showed significant improvement in quality of life and reduction in recurrence of symptomatic atrial fibrillation and associated hospital admissions, suggesting its feasibility as a first line approach for treating patients with symptomatic atrial fibrillation.
Integrated, primary care centered model of care
Like many other chronic diseases, atrial fibrillation can be managed effectively in the primary care setting, often through engagement with specialty and support services. Among the most established models for integrated care are the thrombosis or anticoagulation clinics that are responsible for INR monitoring and dose adjustment of warfarin anticoagulation under the direction of or in collaboration with primary care. Although the role for these clinics may be diminished with the widespread adoption of DOACs, in some instances they remain a resource for collaborative atrial fibrillation care regarding medication safety more generally.160
Beyond anticoagulation, engagement of specialty cardiology or electrophysiology is often necessary. Common reasons for referral include failure of an initial rate control approach, frequent paroxysms of symptomatic atrial fibrillation, persistently elevated heart rate, or intolerance of rate controlling drugs. A first line rhythm control approach may be considered necessary in some patients, and these patients should be evaluated in specialty cardiology or electrophysiology clinics. Rhythm control, particularly with an ablation based approach, has shown consistent benefits in patients with pre-existing heart failure or presumed tachycardia induced cardiomyopathy at the time of presentation with atrial fibrillation.155161 In addition, antiarrhythmic drugs may often be started under specialty care given the need for monitoring at initiation, presence of many drug-drug interactions, and risk of serious cardiac and non-cardiac toxicities. The timing of referral may be determined on a case by case basis, but some data suggest that early referral for consideration of rhythm control may be associated with improved long term control of atrial fibrillation.162 Patients presenting with atrial fibrillation and thromboembolism or other high risk features, such as syncope, angina, or slow ventricular rate may also benefit from early specialty consultation and advanced therapies. Clinicians may consider specialty referral for the conditions and scenarios listed in box 1.
Indications for referral to specialty care
Initial rate control approach has failed or is not well tolerated
First line rhythm control approach is being considered
Pre-existing or newly diagnosed concomitant structural heart disease, such as moderate or severe valvular dysfunction, amyloidosis, hypertrophic cardiomyopathy, or congenital heart defect.
Suspicion of significant coronary artery disease based on clinical history or objective testing
Recent syncope
Atrial fibrillation with slow ventricular rate (<40 bpm) or conversion pauses from atrial fibrillation to sinus rhythm exceeding 3 s or with associated symptoms
Stroke, transient ischemic attack, or peripheral embolism at the time of initial presentation
Young patients (<65 years of age) with new atrial fibrillation
Complex anticoagulation decision making in atrial fibrillation patients at high risk of bleeding, such as those with cerebral amyloid angiopathy—consider left atrial appendage closure
Patient or clinician preference
Although several subspecialists are involved in the care of most atrial fibrillation patients, the primary care setting is central in the longitudinal monitoring and follow-up. With easier access compared with subspecialty clinics, people with atrial fibrillation have a more direct path to primary care to report breakthrough symptoms and revise the treatment plan when necessary. To maximize convenience for patients, routine follow-up for atrial fibrillation may not always necessitate in-person visits. Both atrial fibrillation symptoms and rhythm can be monitored virtually with online patient questionnaires, smartwatch enabled rhythm monitoring, and ambulatory patch rhythm monitoring. The primary care clinician may also be the first contact for a patient experiencing an atrial fibrillation related complication, such as a neurologic event or heart failure decompensation.
An integrated system that facilitates quick interaction between patients, primary care clinicians, and specialized clinics can efficiently adjust the treatment plan to meet the patient’s needs and streamline care (fig 4). In such a system, the primary care clinician can be compared to the quarterback coordinating a team including the cardiologist or electrophysiologist, the neurologist, the anticoagulation expert, and the sleep specialist, among others. Central to such a system are also trained nurses who can directly liaise with the patient, provide education, and help them to interact with specialists and navigate the care system in a way that is minimally disruptive for the patient. In addition to promoting satisfaction among patients and clinicians, such models may reduce cardiovascular and all cause mortality.163164 The 2016 European Society of Cardiology guidelines adopted and promoted a structured multidisciplinary approach to care as the recommended approach to management of atrial fibrillation.165

Model for integration of primary and specialty/multidisciplinary care for atrial fibrillation. AV=atrioventricular; LAAO=left atrial appendage occlusion; RN=registered nurse
{kind=link}
Monitoring and follow-up of atrial fibrillation should include ongoing assessment of the progress with lifestyle recommendations. Feedback from our atrial fibrillation patient reviewers suggests that treating clinicians sometimes place little emphasis on lifestyle counseling. The role of risk factor control, such as weight loss, cardiometabolic fitness, blood pressure reduction, and obstructive sleep apnea management has been well established in the past decade. Abstinence from alcohol was recently shown to reduce atrial fibrillation episodes among regular drinkers with atrial fibrillation in a randomized trial.166 Patients actively engaged in comprehensive risk factor management programs have fewer atrial fibrillation related symptoms, higher quality of life scores, and improved rhythm control after catheter ablation.3637 The unpredictable sustainability of these lifestyle interventions can challenge their long term effectiveness. Longitudinal engagement and reinforcement of their value is therefore important in the primary care setting.
For patients taking antiarrhythmic drugs, routine monitoring for adherence, efficacy, and toxicities is important. For sotalol and dofetilide, patients should undergo evaluation of the QTc interval and renal function every six months.64167 For patients on long term amiodarone, any opportunity should be taken for clinical screening for symptoms or signs of hepatic, thyroid, pulmonary, skin, and eye toxicities. Guidance on laboratory monitoring varies across practices, but hepatic and thyroid function should be assessed six months after drug initiation and every six to 12 months thereafter. Pulmonary function should be assessed annually. Patients should be referred for eye examination annually. Patients should also undergo electrocardiography at least annually to assess for sinoatrial or conduction system dysfunction related to amiodarone. Amiodarone also prolongs the QTc interval in most patients, but unlike other QT interval prolonging drugs, this effect is very rarely torsadogenic.64168
Ongoing research continues to highlight the importance of a multifaceted approach that considers all of the above aspects in patients with atrial fibrillation. For example, in the recently proposed ABC pathway, the “A” criterion is fulfilled if the patient has a time in the therapeutic anticoagulation range of 70% or higher, the “B” criterion is fulfilled if the patient has two or fewer atrial fibrillation related symptoms, and the “C” criterion is fulfilled if the patient is properly managed for the concomitant comorbidities. Atrial fibrillation care in accordance with this pathway was recently shown to be associated with 30-40% lower risk of the composite outcome of all cause hospital admission and death in a complex atrial fibrillation population.169 The same ABC pathway was also recently evaluated in a randomized trial comparing integrated care based on a mobile atrial fibrillation application with usual care in patients with atrial fibrillation.170 The rates of ischemic stroke/systemic thromboembolism, death, and readmission to hospital were lower with the ABC intervention compared with usual care (1.9% v 6.0%; hazard ratio 0.39, 0.22 to 0.67; P<0.001). Mobile technologies may facilitate multifaceted care for complex patients.
Shared decision making with patients
Patient centered care should promote shared decision making in difficult clinical scenarios.171 Patient centered care can be defined as “care that is respectful of and responsive to individual patient needs, values, and preferences” and that ensures “the patient’s values guide all clinical decisions.”172173 Discussions about anticoagulation, especially in older patients with increased risk of bleeding, can be complicated and time consuming.
The goals of atrial fibrillation care need to be established early in the disease course between patient and clinician. The key priority is the prevention of thromboembolism, and clinicians should ensure that patients are well informed and aware of the rationale for anticoagulation. A recent European survey of patients with atrial fibrillation showed that one in 10 patients thought that their anticoagulant would treat the arrhythmia rather than lower their risk of stroke.174 In another survey in the US, almost two thirds of atrial fibrillation patients were not aware that atrial fibrillation is associated with an increased risk of stroke.175 The frequent interactions and established relationship of trust between a patient and his or her primary care provider make primary care the ideal setting for such misconceptions to be tackled. In terms of arrhythmia control, this becomes a priority in patients with highly symptomatic atrial fibrillation and in those with heart failure related to their atrial fibrillation. Despite major advances in the treatment of atrial fibrillation, it has no cure. The goals of antiarrhythmic drugs and ablation procedures are to reduce symptoms and recurrences of atrial fibrillation rather than to cure atrial fibrillation; most patients will have recurrent arrhythmia even after any antiarrhythmic intervention. Realization of these limitations of current treatment modalities can help patients to better align their own goals and expectations and promote a lasting therapeutic interaction with their clinician.
Guidelines
Table 2 summarizes the major guideline recommendations from the American societies (AHA/ACC/HRS) as well as the European societies (the European Society of Cardiology, the European Association for Cardiothoracic Surgery, and the European Heart Rhythm Society).64176 The table includes a summary of the recommendations on screening for atrial fibrillation, the threshold for starting of oral anticoagulation, choice of anticoagulant, treatment after percutaneous coronary intervention (dual versus triple antithrombotic therapy), indications for catheter ablation for atrial fibrillation, and indications for left atrial appendage closure. General agreement exists between organizations for most recommendations. However, the European guidelines give slightly stronger recommendations than the US guideline for anticoagulation for intermediate risk patients (class Ia for patients with a CHA2DS2-VASc score of 1 (male) or 2 (female) versus a class Ib recommendation for CHA2DS2-VASc score ≥1 in men or ≥2 in women), for earlier de-escalation from triple to double therapy after percutaneous coronary intervention (class I recommendation for early cessation of aspirin and continuation of dual therapy following uncomplicated percutaneous coronary intervention versus a IIa recommendation for continued triple therapy for four to six weeks in the US guideline), and for catheter ablation in patients with persistent or longstanding persistent atrial fibrillation refractory to antiarrhythmic drugs (class I versus class IIa and IIb, respectively) or before antiarrhythmic drugs (class IIa versus IIb for longstanding persistent atrial fibrillation).
Comparison of guideline recommendations from 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society (AHA/ACC/HRS) and European Society of Cardiology/European Association for Cardiothoracic Surgery (ESC/EACTS) for management of atrial fibrillation (AF)
Emerging treatments
Although the landscape of antiarrhythmic drugs has not changed significantly in recent years, the field of catheter based ablation treatments for management of atrial fibrillation is rapidly evolving. The long term effectiveness of pulmonary vein isolation, the cornerstone of the ablative management of atrial fibrillation, is limited by the ability to generate transmural and durable atrial lesions. Achieving such lesions requires prolonged and high energy ablation that carries a risk of complications including pulmonary vein stenosis and damage to collateral structures (esophagus, phrenic nerve). A considerable amount of pre-clinical and early clinical data are being generated with the use of alternative catheter ablation energy types, such as pulsed field ablation (or electroporation). Pulsed field ablation has the potential advantage of tissue selectivity such that ablation energy results in desirable atrial myocardial injury, rather than collateral tissue damage. The first few published studies indicate favorable effectiveness and safety profile compared with conventional radiofrequency energy,177178 but more data from larger and longer term multicenter studies are eagerly anticipated in the next one or two years. Eventually, ablation of atrial fibrillation may be achieved without an invasive catheter based approach, instead using technologies used in radiation oncology to deliver precise ablative radiation with stereotactic body radiation therapy. Early experience with ablation of ventricular arrhythmias has shown promise.179
Conclusion
The global burden of atrial fibrillation is rapidly increasing with our aging population and improved screening using wearable technology such as smartwatches. More studies may be needed to support the benefit of identifying and anticoagulating patients with atrial fibrillation detected through screening in preventing thromboembolic strokes. The availability of DOACs has significantly improved adherence to anticoagulation in patients with atrial fibrillation owing to their ease of use and improved safety. Although ablation of atrial fibrillation is recommended in patients with drug refractory symptoms, mounting data support increased success of the procedure with early intervention. With improved catheter designs and safety of existing atrial fibrillation ablation techniques, future studies may need to look at outcomes of early electrophysiological intervention in patients with asymptomatic screen detected atrial fibrillation as opposed to observation and rate control.
Research questions
How might clinicians screen targeted populations at risk for new or undetected atrial fibrillation in a way that is cost effective and minimally disruptive?
What is the optimal stroke prevention strategy in patients at high risk for bleeding who cannot tolerate oral anticoagulation (for instance, patients with cerebral amyloid angiopathy)?
Will novel and emerging ablation techniques improve the efficacy of atrial fibrillation catheter ablation for arrhythmia control and reduction of cardiovascular events?
What is the best approach to the management of patients with atrial fibrillation detected incidentally by implanted cardiac devices (pacemakers or implantable cardioverter-defibrillators, for instance)?
Can formal shared decision making processes improve atrial fibrillation care?
Patient involvement
We engaged a group of patient stakeholders (seven patients in total with one “lead” spokesperson) with atrial fibrillation to review and offer guidance on this manuscript. We identified these patients through the “Mayo Clinic Connect” platform, an online community in which patients can share their experiences and find support. An earlier draft of the manuscript was shared with the patient stakeholders for their review and feedback. Some of the main themes that emerged were:
Striking data on common knowledge gaps, such as that atrial fibrillation is a risk factor for stroke and that anticoagulants do not treat the arrhythmia itself
The critical role of primary care in coordinating the often complex problems that atrial fibrillation patients are faced with
Implications of asymptomatic atrial fibrillation
Perspectives on the importance of widespread availability of and longstanding experience with anticoagulant reversal as a key factor in preferring warfarin over direct acting oral anticoagulants (DOACs)
Challenges with affordability of DOACs
Limited emphasis placed on lifestyle counseling by primary care clinicians and cardiologists caring for atrial fibrillation patients
Acknowledgments
We thank the patient stakeholders (ML and MJ) and Mayo Clinic Connect for helping us to incorporate the patient’s voice and perspective in the drafting and revision of this manuscript.
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Contributors: SPP made substantial contributions to the design and initial drafting of the work (first complete draft), revising it critically for important intellectual content. KCS made substantial contributions to the conception or design of the work, revising it critically for important intellectual content. DRR, JGR, VM, and PAN made substantial contributions to the conception or design of the work, revising it critically for important intellectual content. All authors give final approval of the version to be published and are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. PAN is the guarantor.
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: None.
Provenance and peer review: Commissioned; externally peer reviewed.