Care guided by tissue oxygenation and haemodynamic monitoring in off-pump coronary artery bypass grafting (Bottomline-CS): assessor blind, single centre, randomised controlled trial
BMJ 2025; 388 doi: https://doi.org/10.1136/bmj-2024-082104 (Published 24 March 2025) Cite this as: BMJ 2025;388:e082104Linked Editorial
Near-infrared spectroscopy in perioperative medicine

- Jiange Han, chief physician and chair1,
- Wenqian Zhai, associate chief physician1,
- Zhenhua Wu, chief physician and chair2,
- Zhao Zhang, resident physician1,
- Tao Wang, attending physician1,
- Min Ren, assistant professor3,
- Ziyue Liu, associate professor4,
- Daniel I Sessler, professor and vice president5,
- Zhigang Guo, chief physician and, president6,
- Lingzhong Meng
 , professor and vice chair7,
, professor and vice chair7, - the Bottomline-CS investigation group
- 1Department of Anesthesiology, Tianjin Chest Hospital, Tianjin University, Tianjin, China
- 2Department of Critical Care, Tianjin Chest Hospital, Tianjin University, Tianjin, China
- 3Tianjin Research Institute of Cardiovascular Disease, Tianjin, China
- 4Department of Biostatistics and Health Data Science, Indiana University School of Medicine, Indiana University, Indianapolis, IN, USA
- 5Department of Anesthesiology and Center for Outcomes Research, UTHealth, Houston, TX, USA
- 6Department of Cardiovascular Surgery, Tianjin Chest Hospital, Tianjin University, Tianjin, China
- 7Department of Anesthesia, Indiana University School of Medicine, Indianapolis, IN, USA
- Correspondence to: L Meng menglz{at}iu.edu (@LZMeng1 on x.com)
- Accepted 3 February 2025
Abstract
Objective
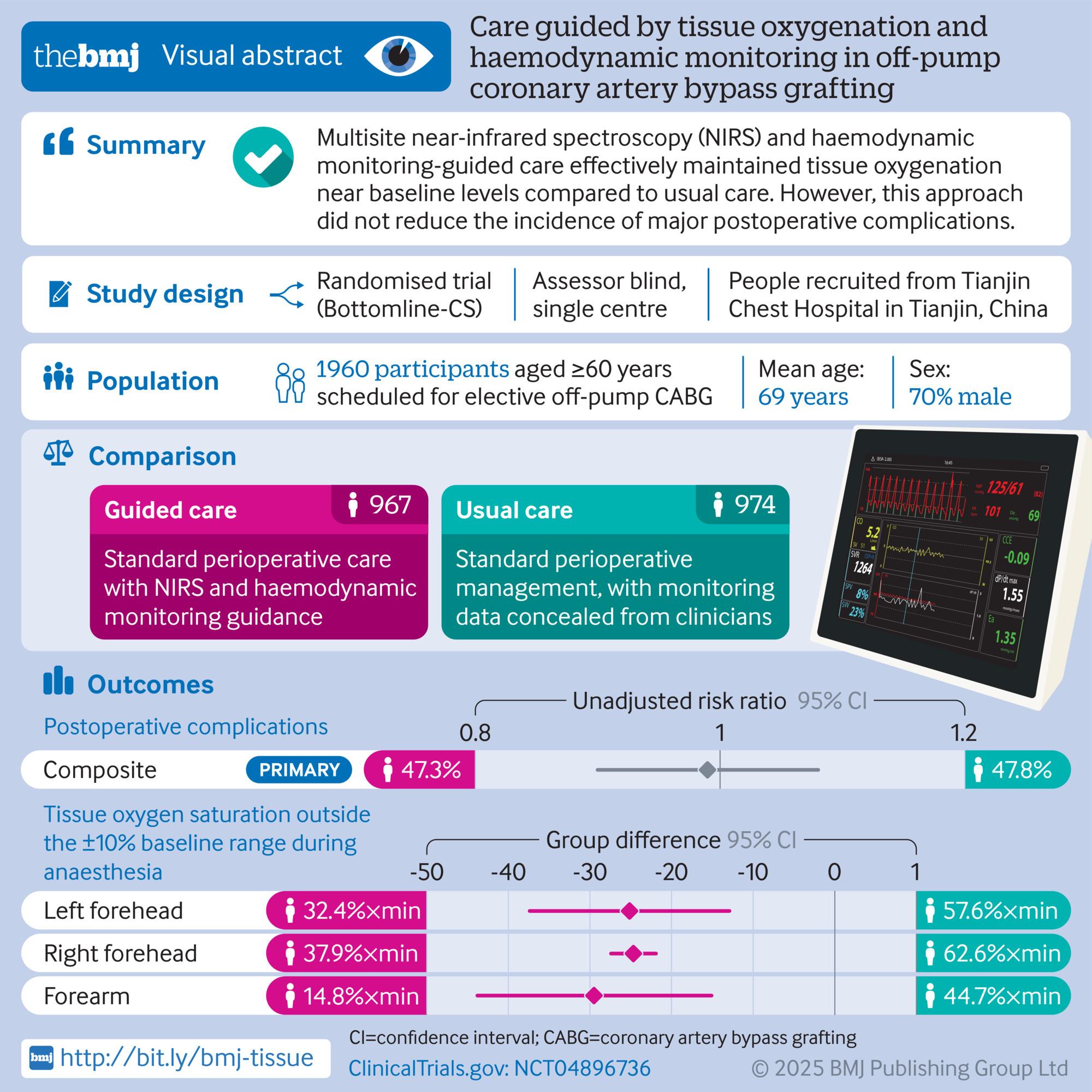
To assess whether perioperative management guided by near-infrared spectroscopy to determine tissue oxygen saturation and haemodynamic monitoring reduces postoperative complications after off-pump coronary artery bypass grafting.
Design
Assessor blinded, single centre, randomised controlled trial (Bottomline-CS trial).
Setting
A tertiary teaching hospital in China.
Participants
1960 patients aged 60 years or older who were scheduled for elective off-pump coronary artery bypass grafting.
Interventions
All patients had multisite monitoring of tissue oxygen saturation (bilateral forehead and unilateral forearm brachioradialis) and haemodynamic monitoring. Both groups received usual care, including arterial blood pressure, central venous pressure, electrocardiography, and transoesophageal echocardiography when indicated. Guided care aimed to maintain tissue oxygenation within 10% above or below preoperative baseline values, established 24-48 hours before surgery, from the start of anaesthesia until extubation or for up to 24 hours postoperatively. In the usual care group, tissue oximetry and haemodynamic data were concealed, and care was routine.
Main outcome measures
The primary outcome was the incidence of a composite of 30 day postoperative complications, which were cerebral, cardiac, respiratory, renal, infectious, and mortality complications. Secondary outcomes included the individual components of the composite outcome, new-onset atrial fibrillation, and hospital length of stay.
Results
Of 1960 patients randomly assigned, data from 967 guided care and 974 usual care patients were analysed. During anaesthesia, the area under the curve for tissue oxygen saturation measurements outside the plus and minus 10% baseline range was significantly smaller with guided care than only usual care: left forehead 32.4 versus 57.6 (%×min, P<0.001), right forehead 37.9 versus 62.6 (P<0.001), and forearm 14.8 versus 44.7 (P<0.001). The primary composite outcome occurred in 457/967 (47.3%) patients in the guided care group and 466/974 (47.8%) patients in the usual care group (unadjusted risk ratio 0.99 (95% confidence interval 0.90 to 1.08), P=0.83). No secondary outcomes differed significantly between groups. The largest observed difference was in incidence of pneumonia, which was less frequent in the guided care group (88/967, 9.1%) than in the usual care group (121/974, 12.4%) and not statistically significant after adjusting for multiple comparisons.
Conclusions
Guided care by use of multisite near-infrared spectroscopy and haemodynamic monitoring effectively maintained tissue oxygenation near baseline levels compared with usual care. However, no clear evidence was noted that this approach reduced the incidence of major postoperative complications. These findings do not support the routine use of near-infrared spectroscopy and haemodynamic monitoring to maintain tissue oxygenation during off-pump coronary artery bypass grafting.
Trial registration
ClinicalTrials.gov NCT04896736.

{kind=link}
Introduction
Complications following cardiac surgery are both common and serious, including postoperative delirium in 12% of cases,1 cognitive decline in 47%,2 cardiac complications in 49.5%,3 atrial fibrillation in 34%,1 acute kidney injury in 22%,4 respiratory failure in 16%,5 major infections in 5%,6 and in-hospital mortality in 3.4%.7 Consequently, the likelihood of having one or more major complications after cardiac surgery is substantial. A key contributor to these complications is inadequate tissue perfusion or organ hypoperfusion.8 9 Optimal haemodynamic management has shown promise in reducing complications, particularly in non-cardiac surgeries.10 11 12 13 14 However, perioperative haemodynamic management often relies solely on blood pressure monitoring despite its poor correlation with tissue perfusion.8 15 16 17 Therefore, an approach centred around blood pressure might not ensure adequate oxygen delivery to tissues.
Tissue oximetry based on near-infrared spectroscopy offers a non-invasive method to estimate tissue oxygen saturation, reflecting the balance between oxygen delivery and consumption in the tissue bed.8 18 19 20 21 22 This technology enables real-time monitoring of tissue perfusion related physiology, allowing clinicians to intervene before adverse outcomes develop. Cohort studies have linked tissue desaturation to worse postoperative outcomes, supporting its use in guiding perioperative care.23 24 However, randomised trials have yielded inconsistent results.25 26 These trials were often small (the largest enrolling 249 patients), inadequately powered, and focused solely on cerebral tissue oxygen saturation—potentially overlooking perfusion deficits in non-cerebral tissues.25 26 Different tissue beds respond variably to haemodynamic stresses,27 underscoring the importance of comprehensive, multisite tissue monitoring. Furthermore, the absence of continuous haemodynamic monitoring in prior trials limited clinicians’ ability to identify and address perfusion deficits effectively.
Given these limitations, larger trials are needed to comprehensively monitor tissue oxygenation across multiple sites while integrating continuous real-time haemodynamic data to facilitate differential diagnoses. In this study, we tested the hypothesis that perioperative care guided by cerebral (SctO2) and somatic (SstO2) tissue oxygen saturation, combined with real-time haemodynamic monitoring, reduces the incidence of a composite of 30 day postoperative complications in patients undergoing off-pump coronary artery bypass grafting (CABG). Secondary outcomes included the individual components of the primary composite, the incidence of atrial fibrillation, and the duration of hospitalisation.
Methods
Trial design
The Bottomline-CS (better outcome through tissue oxygenation monitoring linked with intervention in cardiac surgery) trial was an assessor blinded, single centre, randomised trial comparing perioperative care guided by multisite tissue oxygen saturation and haemodynamic monitoring with usual care in patients having elective off-pump CABG. We selected off-pump CABG due to the resultant unique haemodynamic challenges, particularly the substantial disturbances caused by heart manipulation and positioning during the procedure. These disturbances, characterised by extreme hypotension and hypertension (supplementary figure 1), closely mimic real-world clinical scenarios where severe haemodynamic fluctuations risk poor outcomes for patients. Additionally, enrolment was restricted to patients undergoing off-pump CABG because more than half of CABG procedures in Asia are performed without cardiopulmonary bypass.28
Our trial received approval from the internal review board of Tianjin Chest Hospital on 30 March 2021. Tianjin Chest Hospital, a tertiary teaching hospital affiliated with Tianjin University, is located in Tianjin, China. The hospital performs over 3000 cardiac procedures annually, including more than 1600 off-pump CABGs, making it the third highest in China for CABG volume. Written informed consent was obtained from participants at least 24 h before surgery. The trial was registered at ClinicalTrials.gov (NCT04896736) before enrolment of the first patient. This report adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Participants
Patients aged 60 years or older who were scheduled for elective off-pump CABG were considered eligible. Exclusion criteria included preoperative dependence on respiratory support, use of an external cardiac assist device, urgent or emergent surgery, and an expected mortality within 30 days.
Protocol and interventions
One to two days before surgery, baseline measurements of SctO2 at the left and right forehead and SstO2 at the forearm brachioradialis were recorded for all participants. Tissue oxygen saturation was assessed using near-infrared spectroscopy cerebral and tissue oximetry (Nonin Medical, Plymouth, MN, USA). Measurements were conducted in hospital rooms with patients in a supine position, awake, calm, with eyes closed, and breathing either room air or their usual home oxygen. Concurrently, non-invasive estimations of cardiac output, stroke volume, systemic vascular resistance, heart rate, and blood pressure were obtained using a finger and arm cuffs-based haemodynamic monitor (continuous non-invasive arterial pressure module, Masimo LiDCO Haemodynamic Monitoring System, Masimo, Irvine, CA, USA).
In the operating room, patients’ haemodynamic parameters were routinely monitored, including continuous arterial blood pressure via a radial artery catheter, continuous central venous pressure via a central venous catheter inserted through the internal jugular vein, electrocardiography, and transoesophageal echocardiography when indicated. Anaesthesia was induced with either propofol or etomidate and maintained using propofol infusion or sevoflurane inhalation, or both, with the choice of anaesthetics determined by the attending anaesthesiologists. Cisatracurium or rocuronium was used for muscle relaxation. All patients were intubated and mechanically ventilated. Sufentanil served as the main analgesic intraoperatively and postoperatively, per institutional routine. Postoperative sedation, when required, was administered with propofol, midazolam, or dexmedetomidine at the discretion of the managing intensivists.
All trial participants received continuous multisite tissue oxygen saturation monitoring during and after surgery, using the same locations and technology as the preoperative measurements (Nonin Medical, Plymouth, MN, USA). Simultaneously, participants had continuous haemodynamic monitoring with a minimally invasive system (Masimo LiDCO Haemodynamic Monitoring System, Masimo, Irvine, CA, USA). This system estimated haemodynamic variables from the arterial blood pressure waveform transmitted from an intra-arterial catheter placed in the radial artery, differing from the non-invasive finger and arm cuffs-based technology used for preoperative assessment.
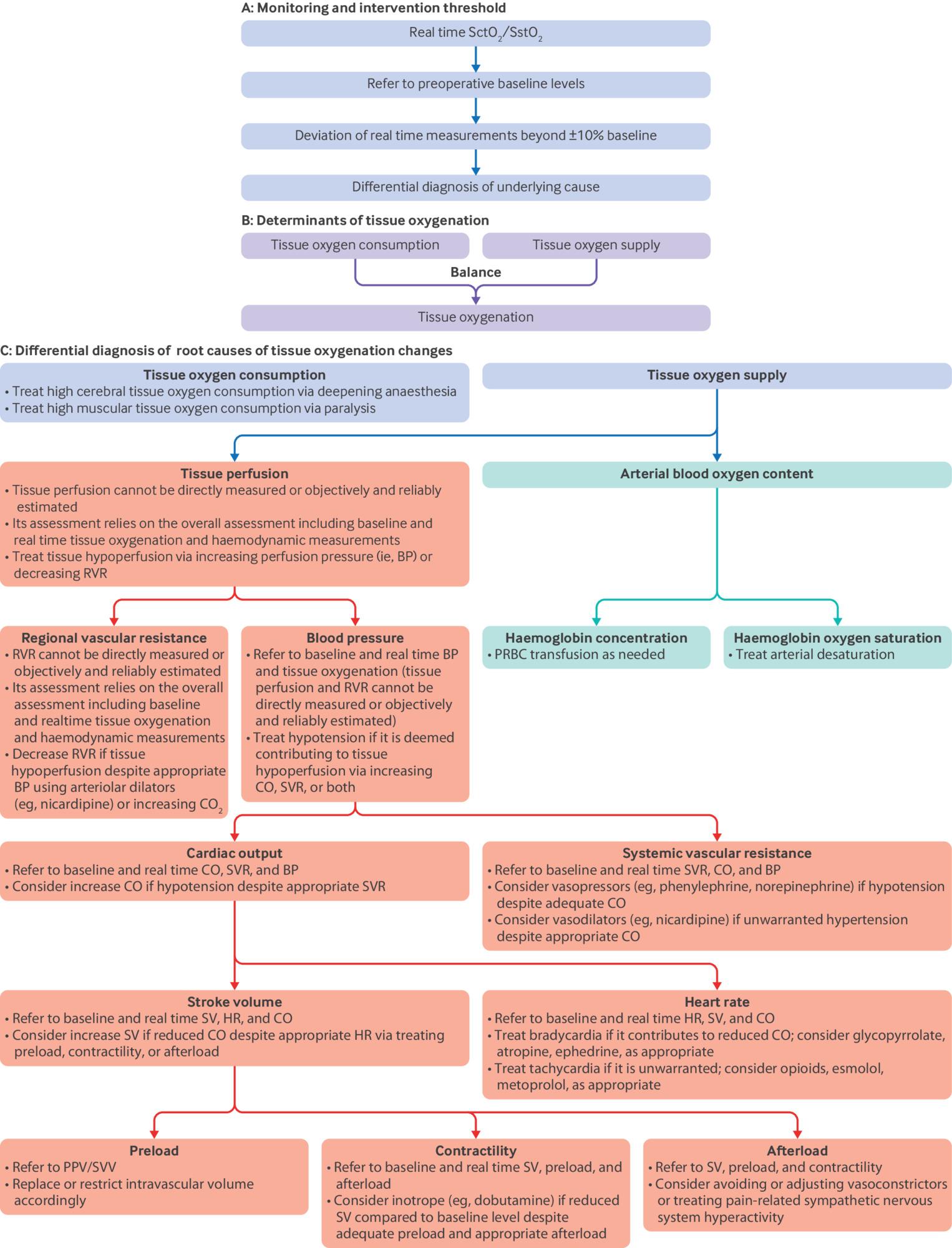
In patients assigned to guided care, the goal was to keep forehead SctO2 and forearm SstO2 within ±10% of individual preoperative baseline values, measured in hospital rooms 24-48 h before the scheduled CABG.24 Tissue oxygen saturation reflects the balance between oxygen delivery and consumption, with delivery determined by perfusion and arterial oxygen content. Managing physicians addressed deviations in tissue oxygenation by focusing on three domains: tissue perfusion, arterial oxygen content, and oxygen consumption (fig 1).

Multisite tissue oxygenation and haemodynamic monitoring intervention protocol. The protocol for managing patients having off-pump coronary artery bypass grafting using multisite tissue oxygenation and haemodynamic monitoring. Red boxes indicate haemodynamics, green indicate arterial blood oxygen content, and purple indicate tissue oxygen consumption and supply. The objective was to maintain SctO2 at the left and right forehead and SstO2 at the forearm within 10% higher or lower than the patient's baseline values from intubation until extubation or 24 h after surgery (A). Tissue oxygenation is determined by the balance between tissue oxygen consumption and supply (B). The figure illustrates the complex, multifactorial causes of deviations in SctO2 and SstO2 and emphasises the critical role of comprehensive differential diagnosis in clinical management (C). The protocol also underscores the hierarchical relationship and integration of haemodynamic parameters—including CO, SV, and SVR—into clinical decision making, ensuring a more holistic approach rather than focusing on isolated variables. Baseline haemodynamic and tissue oxygenation values were pivotal in diagnosing the underlying causes of deviations and guiding precise interventions. BP=blood pressure; CO=cardiac output; CO2=carbon dioxide; HR=heart rate; PPV=pulse pressure variation; PRBC=packed red blood cell; RVR=regional vascular resistance; SctO2=cerebral tissue oxygen saturation; SstO2=somatic tissue oxygen saturation; SV=stroke volume; SVR=systemic vascular resistance; SVV=stroke volume variation
{kind=link}
Simultaneous haemodynamic monitoring, including cardiac output, stroke volume, and systemic vascular resistance, was used to diagnose the underlying causes of tissue oxygenation changes (fig 1). Rather than prescribing specific treatments, we recommended a bundle of potential interventions tailored to address the various causes of tissue desaturation and hypersaturation (ie, unwarranted increase or decrease). Providers managing trial participants were well trained, having practised the intervention protocol in at least 20 patients before the study. The intervention period began with anaesthesia induction and continued until extubation in the intensive care unit or up to 24 h postoperatively.
In patients randomly assigned to usual care, clinicians managed haemodynamics using standard monitoring, which included continuous arterial blood pressure via a radial artery catheter, central venous pressure via a central venous catheter inserted through the internal jugular vein, electrocardiography, and transoesophageal echocardiography when clinically indicated. Although these patients were also monitored with near-infrared spectroscopy tissue oximetry and LiDCO haemodynamic system, clinicians were blinded to the data from both monitors.
Outcomes
The primary outcome was a composite of one or more serious complications occurring within 30 days postoperatively. These were cerebral complications (ie, postoperative delirium, cognitive decline, or stroke), cardiac complications (ie, non-fatal cardiac arrest, myocardial injury, heart failure, or newly diagnosed symptomatic ventricular arrhythmia), respiratory failure, renal injury (ie, acute kidney injury stages II or III), infections (ie, deep surgical site or organ/space infection, pneumonia, confirmed bloodstream infection, uncertain source infection, or sepsis), and mortality. Each component required at least a Clavien-Dindo grade II classification (necessitating clinical intervention).29 Secondary outcomes comprised the individual components of the primary outcome, atrial fibrillation within 30 days, and the duration of hospital stay. Detailed diagnostic criteria are provided in supplementary table 1.
Patients were assessed twice daily after surgery until discharge. Investigators also interviewed family members and care givers to gather relevant information. Post-discharge outcomes were evaluated at a follow-up visit, typically on day 30, or by phone if an in-person visit was not feasible. Any uncertainties or discrepancies in outcome assessments were resolved through consensus.
Randomisation and blinding
Patients were randomised 1:1 to guided or usual perioperative care using computer generated allocations in blocks of four, accessed via a secure website on the morning of surgery. The individual responsible for generating the random allocations did not participate in intraoperative management or postoperative outcome assessment. Near-infrared spectroscopy tissue oxygenation and LiDCO haemodynamic data were accessible to clinicians managing patients in the guided care group, while these data were concealed from clinicians managing the usual care group.
Managing anaesthesiologists during surgery and intensivists after surgery were not masked to group assignments due to the study design. However, outcome assessors were independent, uninvolved in perioperative care, and masked to group assignments. Patients were not informed of their allocation. Oversight bodies, including the trial steering committee, remained masked throughout enrolment. The independent data monitoring committee reviewed interim data by group without knowing the group identities.
Sample size
The sample size calculation assumed that 30% of patients receiving usual care would have the primary composite outcome, compared with 24% in the group managed with multisite tissue oxygen saturation and haemodynamic monitoring—a 20% relative reduction deemed clinically meaningful. We used a one sided group sequential Z testing with three stages, including two interim analyses. Boundary values for efficacy were based on the O'Brien-Fleming α-spending function, while a non-binding β-spending function was used for futility.
The required sample size was 927 patients per group to achieve 80% power to detect a 6% absolute reduction in the primary outcome incidence (from 30% to 24%) at a type I error level of 0.05. Accounting for a 5% anticipated dropout or missing data rate, the target recruitment goal was set at 980 patients per group.
Statistical methods
We finalised a comprehensive statistical analysis plan before unblinding and analysis. Continuous variables were summarised as means with standard deviations (SD) or medians with interquartile ranges (IQR), depending on the distribution. Group comparisons for normally distributed data were conducted using t-tests, while Wilcoxon rank-sum tests were used for non-parametric data. Categorical variables were reported as counts and percentages, with group comparisons made using Pearson’s chi-squared test or Fisher’s exact test, as appropriate. Group differences were assessed using mean or median differences for continuous variables and differences in proportions for categorical variables.
We used a modified intention-to-treat population for the primary analysis, which included all randomly assigned patients with available primary outcome data, regardless of the care they received, unless consent was withdrawn.30 We used log-binomial regression to assess the primary outcome, with treatment allocation as the sole independent variable. Intervention effects were expressed as relative risks with 95% confidence intervals (CI). We defined statistical significance by a one sided Z value of less than −1.932 (P<0.03), consistent with the group sequential design.31 A one-sided test was chosen to evaluate whether guided care improves outcomes compared with usual care. We analysed secondary outcomes using generalised linear models for continuous data and log-binomial regression or chi-squared tests for categorical data. Safety analyses focused on adverse events potentially related to the intervention.
We used post hoc analyses to aid in interpreting the primary composite outcome. These analyses included standard approaches, such as combining events versus no events, event counting, and individual component analyses, as well as advanced methods like multivariate generalised estimating equations, the common effect test, and the average relative effect test.32
Alongside the unadjusted analyses described above, we also performed adjusted analyses for baseline imbalances discovered in the analysis using multivariable log-binomial regression models to account for potential confounders, as prespecified in the statistical analysis plan for primary and secondary outcomes. Baseline homogeneity was assessed with absolute standardised differences, with values exceeding 1.96×√(nt+nc)/(nt×nc) deemed to be imbalanced, where nt and nc represent the sample sizes of the treatment and control groups.33 Post hoc analyses included further adjustments for age, sex, body mass index, and history of diabetes and hypertension using multivariable log-binomial regression models.
Sensitivity analyses were conducted on the per-protocol population, comprising patients who adhered to the guided care or usual care protocol and had primary outcome data available. Adherence to the guided care protocol was defined as maintaining all three tissue oxygen saturation values within 10% higher or lower than the baseline for at least 80% of the surgery duration. Patients were excluded from these analyses if their equipment malfunctioned, they had substantial protocol deviations, they were deemed ineligible, or they underwent cardiopulmonary bypass instead of the planned off-pump surgery.
Additional sensitivity analyses were conducted to address missing primary outcome data. For data assumed to be missing at random, the Markov Chain Monte Carlo method was applied for multiple imputations. Twenty imputed datasets were generated by sampling from the Bayesian posterior distribution to create stationary distribution chains and simulate missing values. For data not assumed to be missing at random, analyses were performed using best-case and worst-case scenarios and selection models.
For the subgroup analyses of the primary outcome, we used the modified intention-to-treat population (excluding patients without primary outcome data). These analyses assessed interactions between the intervention and variables such as age, sex, body mass index, comorbidities, and smoking status. We also evaluated baseline physiological parameters, including tissue oxygen saturation, cardiac output, stroke volume, systemic vascular resistance, heart rate, and mean blood pressure.
The type I error level was set at 0.05 for all analyses. To account for multiple comparisons across the 24 secondary hypotheses, the Holm-Bonferroni method was applied. This stepwise procedure sequentially adjusts P value thresholds based on their rank, ensuring the family-wise error rate remained controlled at 5% while maintaining statistical rigour. Statistical analyses were performed using R (version 4.4.0, R Foundation for Statistical Computing, Vienna, Austria) with the following packages: tableone, dplyr, readxl, grid, forestploter, mice, lme4, and broom.34
Patient and public involvement
Patients were not involved in setting the research question, determining the outcome measures, or developing recruitment and implementation plans. They were also not consulted on the interpretation or reporting of the results. However, patient and family engagement throughout the trial was instrumental in ensuring its successful completion.
Results
Recruitment and participant flow
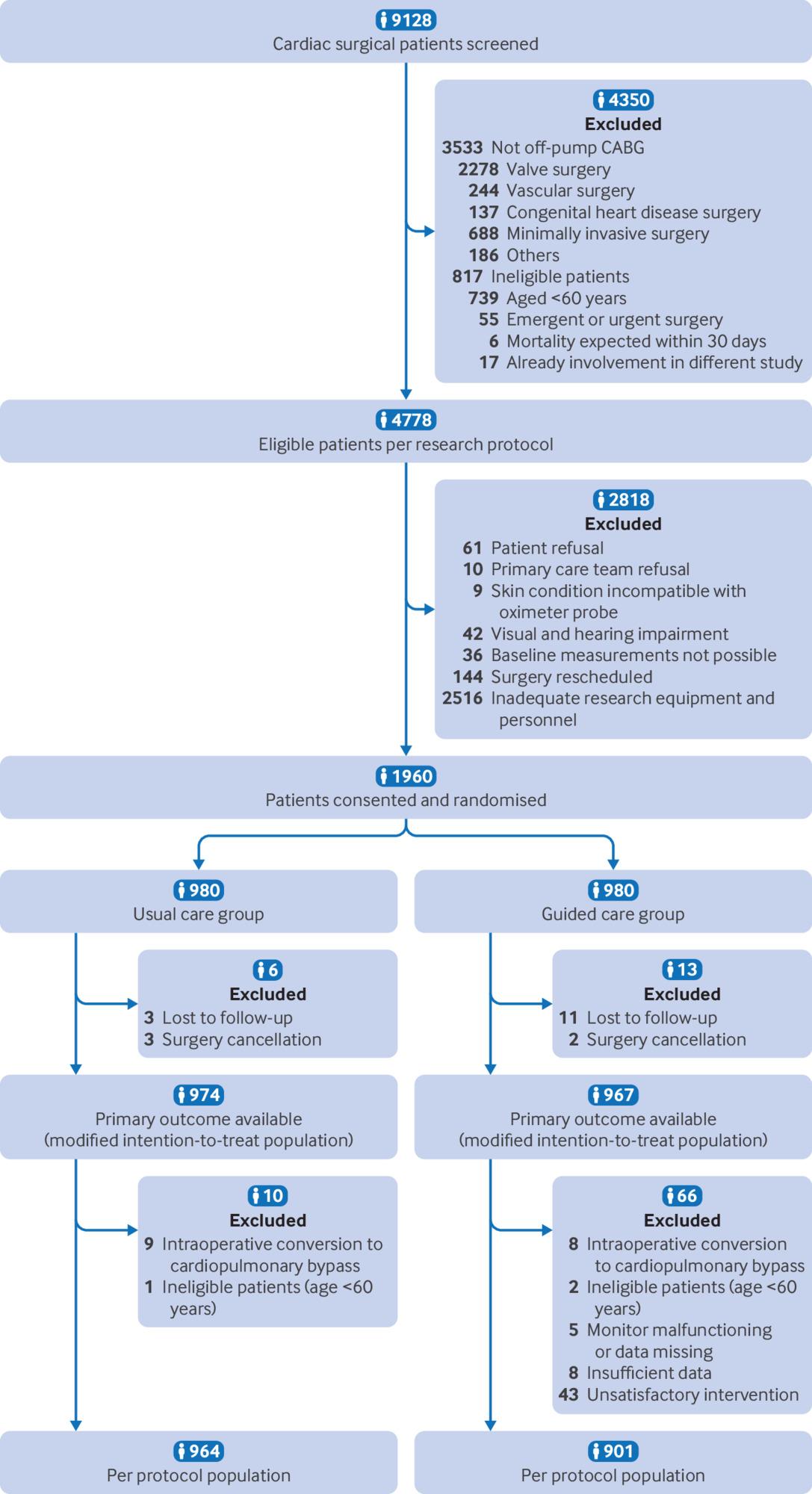
We screened 9128 patients undergoing cardiac surgery between 8 June 2021 and 27 December 2023 of whom 1960 met eligibility criteria and provided consent (fig 2). The data and safety monitoring board reviewed the trial at two interim analyses and did not recommend any protocol amendments or trial discontinuation. An onsite quality audit, requested by the investigators and conducted by the Peking University Clinical Research Institute between 28 February and 2 March 2023, identified no substantive protocol violations or conduct issues.

Recruitment, randomisation, and follow-up in a trial of multisite tissue oxygenation and haemodynamic monitoring guided care in patients having off-pump CABG. CABG=coronary artery bypass grafting
{kind=link}
Following randomisation, 13 patients in the guided care group and six in the usual care group had their surgery cancelled or were lost to follow-up (supplementary table 2). The modified intention-to-treat population ultimately included 967 patients in the guided care group and 974 in the usual care group.
Baseline and perioperative data
The demographic and baseline characteristics of patients in the guided care and usual care groups are summarised in table 1 and supplementary table 3. The calculated threshold for imbalance was 1.96×√(nt+nc)/(nt×nc)=0.089. Among the baseline variables, only systemic vascular resistance (absolute standardised difference 0.091) and haemoglobin concentration (absolute standardised difference 0.108) exceeded this threshold.
Demographic and preoperative baseline characteristics in the modified intention-to-treat population
Expected differences in intraoperative management were observed (table 2). Patients in the guided care group received more midazolam and propofol than in the usual care group, likely to reduce anxiety and stabilise tissue oxygenation and haemodynamics before anaesthesia induction. Reduced sevoflurane use in the guided care group might reflect efforts to maintain lighter anaesthesia, supporting haemodynamic stability. Increased muscle relaxant use in the guided care group were likely aimed to decrease muscle oxygen consumption through paralysis, while higher sufentanil administration might have been intended to attenuate the stress response and stabilise haemodynamics.
Intraoperative and postoperative intervention and laboratory data based on the modified intention-to-treat population
In the guided care group in comparison with the usual care group, increased use of metaraminol and reduced norepinephrine use probably reflect the use of metaraminol boluses for rapid blood pressure restoration, with norepinephrine primarily used as a continuous infusion. Higher tranexamic acid administration was likely aimed to minimise blood loss and maintain haemodynamic stability. Reduced dexmedetomidine use was possibly to avoid bradycardia, reduced cardiac output, and hypotension. Greater fluid administration probably targeted the maintenance of cardiac output and optimisation of tissue perfusion. Reduced blood loss may have been attributable to tranexamic acid use and stable haemodynamics, while lower glucose levels could reflect reduced physiological stress, potentially due to greater haemodynamic stability and increased narcotic use. Postoperatively, reduced esmolol use may have sought to avoid bradycardia, while increased urine output likely related to higher intraoperative fluid administration. We present other intraoperative and postoperative data, which show no significant between-group differences, in supplementary table 4.
Ward baseline, pre-induction, and post-induction measurements of left SctO2, right SctO2, and SstO2 were similar between groups (table 3 and supplementary table 5). During surgery, more patients in the guided care group versus the usual care group maintained tissue oxygen saturation within plus or minus 10% of their ward baseline for at least 80% of the time: 95.1% (907/954) v 60.0% (571/952) (P<0.001) for the left forehead, 95.0% (906/954) v 58.4% (556/952) (P<0.001) for the right forehead, and 95.5% (911/954) v 58.5% (557/952) (P<0.001) for the forearm based on patients who had more than 30 minutes intraoperative monitoring data (table 3). Overall, 95.0% (906/954) of patients in the guided
Baseline and intraoperative tissue oxygenation and haemodynamic data in the modified intention-to-treat population
care group maintained all three tissue oxygen saturations within 10% higher or lower than the ward baseline for at least 80% of the time, compared with 58.4% (556/952) in the usual care group.
During surgery, the area under the curve for tissue oxygen saturation beyond the ±10% baseline range was significantly smaller in the guided care group compared with the usual care group: 32.4 v 57.6% × min (P<0.001) for the left forehead, 37.9 v 62.6% × min (P<0.001) for the right forehead, and 14.8 v 44.7%×min (P<0.001) for the forearm (table 3). However, postoperative tissue oxygenation was similar between groups (supplementary table 6).
Outcomes and estimation
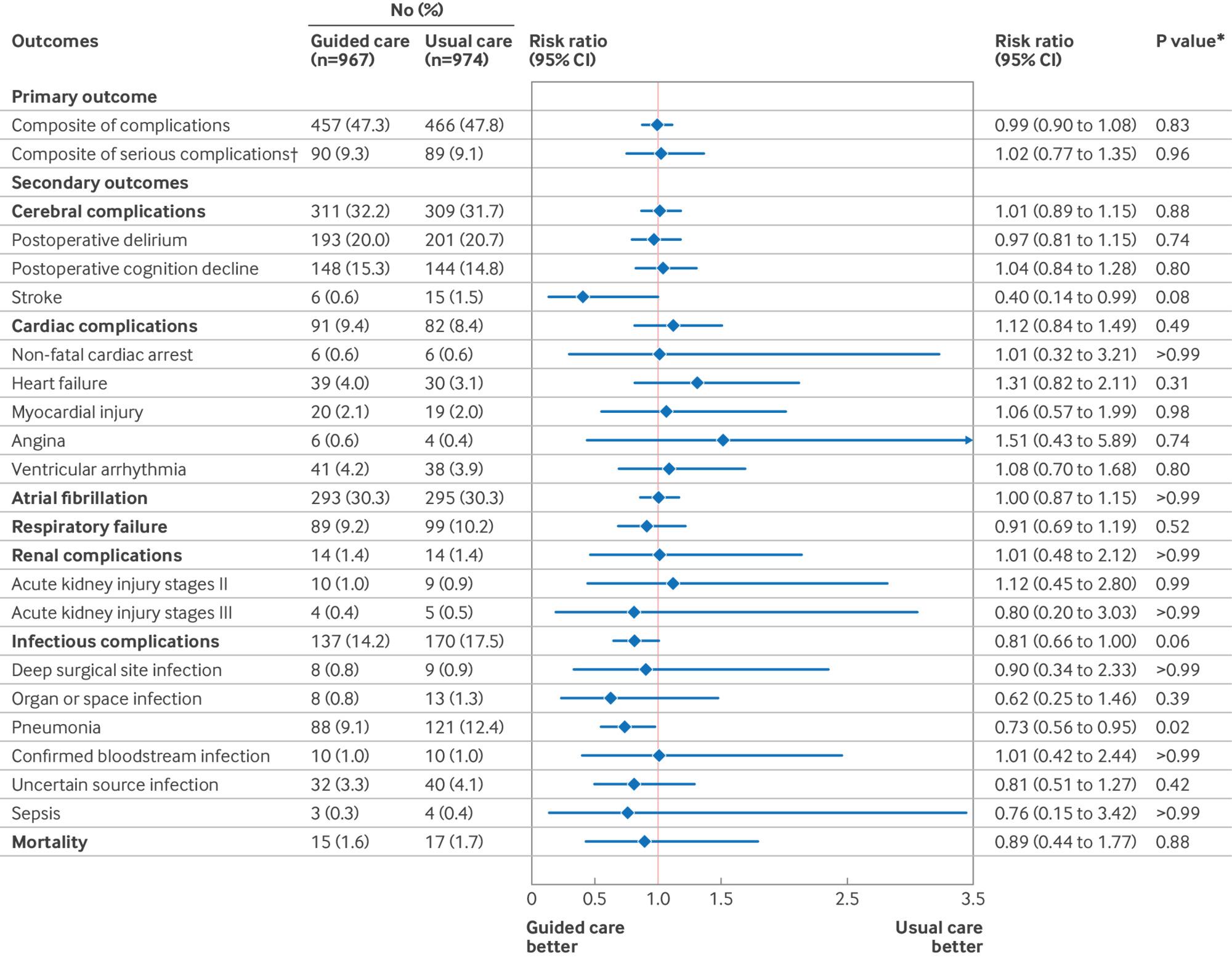
Primary composite complications occurred in 457 (47.3%) of 967 patients in the guided care group and 466 (47.8%) of 974 patients in the usual care group, resulting in an unadjusted risk ratio of 0.99 (95% CI 0.90 to 1.08), P=0.83). After adjustment for baseline imbalances in systemic vascular resistance and haemoglobin concentration, the risk ratio was 0.99 ((95% CI 0.90 to 1.09); P=0.83). A total of 24 secondary hypotheses were tested using multivariable log-binomial regression models, both unadjusted (fig 3) and adjusted for pre-existing imbalances and known prognostic factors (supplementary table 7). None of the secondary analyses showed statistically significant between-group differences after adjustments for multiple comparisons using the Holm-Bonferroni method.

Primary and secondary outcomes based on the modified intention-to-treat population. CI=confidence interval. *None of the P values for secondary outcomes was significant after adjustments for multiple comparisons using the Holm-Bonferroni method. †The post hoc composite of serious complications included stroke, non-fatal cardiac arrest, heart failure, new-onset symptomatic ventricular arrhythmia, acute kidney injury stage III, sepsis, and mortality
{kind=link}
Among the secondary outcomes, the largest observed differences were in pneumonia, infectious complications, and stroke. Pneumonia occurred in 88 (9.1%) of 967 patients in the guided care group and 121 (12.4%) of 974 patients in the usual care group, with an unadjusted risk ratio of 0.73 ((95% CI 0.56 to 0.95), P=0.02 before adjustment for multiple comparisons, P=0.60 after adjustment). Infectious complications occurred in 137 (14.2%) of 967 patients versus and 170 (17.5%) of 974 patients, with an unadjusted risk ratio of 0.81 ((0.66 to 1.00), P=0.06 before adjustment, P>0.99 after adjustment). Stroke occurred in six (0.6%) of 967 patients versus 15 (1.5%) of 974 patients, with an unadjusted risk ratio of 0.40 ((0.14 to 0.99), P=0.08 before adjustment, P>0.99 after adjustment). To account for potential sparse data bias, ad hoc Bayesian log-binomial regression was fitted with a resultant risk ratio of 0.45 (95% CI 0.14 to 1.02).35
The median hospital stay was nine days for both groups. No significant between-group differences were observed in safety outcomes, including intraoperative conversion to on-pump surgery, anaphylactic shock, and postoperative haemorrhage (supplementary table 8).
Ancillary analyses
The per protocol analysis included 901 participants in the guided care group and 964 in the usual care group (supplementary tables 9-15 and supplementary figure 2). The primary composite outcome occurred in 418 (46.4%) of 901 patients in the guided care group and in 460 (47.7%) of 964 patients in the usual care group, yielding an unadjusted risk ratio of 0.97 ((95% CI 0.88 to 1.07), P=0.60). None of the per-protocol secondary analyses, adjusted for multiple comparisons, showed significant between-group differences.
The largest observed differences were in pneumonia, stroke, and infectious complications. Pneumonia occurred in 80 (8.9%) of 901 patients in the guided care group compared with 119 (12.3%) of 964 patients in the usual care group (unadjusted risk ratio 0.72 (95% CI 0.55 to 0.94), P=0.02 before adjustment for multiple comparisons, P=0.49 after adjustment). Stroke occurred in three of 901 patients (0.3%) versus 13 (1.3%) of 964 patients (0.25 (0.06 to 0.76), P=0.03 before adjustment, P=0.88 after adjustment). To account for potential sparse data bias, ad hoc Bayesian log-binomial regression was fitted with a resultant risk ratio of 0.28 ((95% CI 0.05 to 0.75)).35 Infectious complications occurred in 124 (13.8%) of 901 patients versus 168 (17.4%) of 964 patients (0.79 (0.64 to 0.98), P=0.04 before adjustment for multiple comparisons, P=0.91 after adjustment).
Preplanned sensitivity analyses of the primary outcome, based on the intention-to-treat population, produced similar results, with the missing primary outcome data imputed using various methods (supplementary table 16). No differences were found in any preplanned subgroup analyses (supplementary figure 3).
Discussion
Principal findings
A significantly higher proportion of patients in the guided care group maintained intraoperative multisite tissue oxygen saturation within 10% higher or lower than baseline for at least 80% of the surgical period compared with those in the usual care group (95% v 58%). Additionally, the area under the curve beyond the plus or minus 10% baseline range was nearly halved in the guided care group. Patients in the guided care group also had higher overall blood pressure and cardiac output than their usual care counterparts. Exposure was thus well controlled.
Despite these physiological benefits, the incidence of the primary composite outcome did not differ significantly between patients managed with and without near-infrared spectroscopy tissue oxygenation and LiDCO haemodynamic monitoring. None of the primary composite components, including cerebral, cardiac, respiratory, renal, infectious, and mortality complications, showed significant differences. Secondary outcomes, including atrial fibrillation and hospital duration, were also similar. These findings robustly indicate that perioperative care guided by multisite tissue oxygen saturation and haemodynamic monitoring does not reduce the incidence of common postoperative complications following cardiac surgery.
Pneumonia, however, may represent a distinct case. The observed 27% reduction in pneumonia incidence (9.1% v 12.4%) is clinically meaningful. Whether this reduction reflects a true benefit that did not reach statistical significance because of insufficient power or is a spurious finding from multiple comparisons remains uncertain. The spurious finding explanation is more likely. Nevertheless, the potential benefit aligns with results from a network meta-analysis showing that goal directed haemodynamic treatments significantly reduce surgical site infections compared with standard care.13 However, pneumonia differs from surgical site infections in both biological cause and clinical course. Further research is warranted that is specifically designed and adequately powered to evaluate pneumonia as an outcome.
We initially estimated that 30% of patients randomly assigned to usual care would have complications included in the composite outcome. In reality, 47% of patients had one or more such complications. This higher incidence enhanced the power of our trial, resulting in a 95% confidence interval for the primary relative risk of less than 10% within baseline measurements. Similarly, confidence intervals for most secondary outcomes were narrow, reinforcing that our findings are genuinely neutral rather than underpowered.
Comparison with other studies
A systematic review and meta-analysis assessed the impact of intraoperative SctO2-guided care on postoperative delirium and cognitive decline in patients who had cardiac surgery.25 Across six trials involving 947 patients, SctO2 guided management significantly reduced postoperative delirium (odds ratio 0.28 (95% CI 0.09 to 0.84); P=0.02; I2=81%). However, two trials raised eligibility concerns: one, which heavily influenced the positive findings, did not directly assess postoperative delirium,36 and another combined SctO2 monitoring with processed electroencephalography, which complicates interpretation.37 By contrast, a separate meta-analysis of five randomised controlled trials involving 825 patients who had cardiac surgery reported no significant effect of SctO2-guided care on postoperative delirium.38 The systematic review also reported a significant reduction in postoperative cognitive decline (odds ratio 0.38 (95% CI 0.16 to 0.93); P=0.03; I2=78%) based on five trials involving 858 patients.25 Overall, these prior trials were small, with the largest enrolling only 249 patients, and exhibited substantial heterogeneity. Moreover, none used multisite tissue oxygen saturation monitoring or continuous real-time haemodynamic monitoring to guide care. Notably, their confidence intervals were wide, exceeding 0.75, contrasting with the tight interval observed in our trial.
Another trial evaluated care guided by SstO2 (without SctO2) and haemodynamic monitoring in 800 women undergoing laparoscopic hysterectomy, reporting no significant reduction in postoperative nausea and vomiting.39 Similarly, a randomised trial assessed SctO2-guided oxygen delivery in 607 preterm neonates during the immediate post-birth transition.40 This study found no significant improvement in survival without cerebral injury when compared with standard care. Collectively, these findings strongly suggest that care guided by tissue oxygenation monitoring does not consistently yield substantial improvements in meaningful clinical outcomes.
Strengths and limitations of this study
We acknowledge that using SstO2 that is monitored on the forearm brachioradialis to infer outcomes related to distant organs may appear counterintuitive. However, its inclusion in our study design was informed by prior evidence showing that SstO2, but not SctO2, was associated with postoperative outcomes in patients undergoing major spine surgery.23 This rationale was further supported by secondary analyses from this trial, which showed a significant association between higher preoperative SstO2 and a reduced risk of postoperative delirium, whereas SctO2 showed no such association (unpublished data).
The observed differences between SstO2 and SctO2 likely arose from the insensitivity of SctO2 to systemic haemodynamic stresses. Cerebral autoregulation tightly maintains stable cerebral blood flow and brain oxygenation despite systemic fluctuations.27 41 42 By contrast, SstO2 reflects the dynamic balance between oxygen delivery and metabolic demand in peripheral tissues, serving as a marker of systemic physiological reserve and broader vulnerabilities. These findings underscore the potential of SstO2 as a practical, non-invasive biomarker for perioperative risk stratification and its promise as a target for optimisation in perioperative care.
A limitation of our trial is the open label design, necessitated by the nature of the intervention, which may have introduced performance or detection bias. However, we mitigated this risk by masking participants, non-anaesthesia care providers, and outcome assessors. In any trial using usual care as a reference, outcomes are affected by the standard of care at each institution, which can vary significantly due to sparse evidence guiding many aspects of clinical management. Consequently, practices are often shaped by routine rather than strong evidence, potentially affecting the generalisability of our findings to institutions with different clinical practices.
Another limitation is our use of a collapsed composite endpoint (one or more complications within a predefined list), a common approach in perioperative trials.32 While practical, this method can disproportionately emphasise more frequent but less severe outcomes, potentially skewing the overall interpretation of results.32 To address this, we performed additional analyses, which generated similar results.
Restricting enrolment to a single centre ensured consistent care and intervention exposure but limited the generalisability of our findings, as patient populations and medical practices vary across hospitals and regions. While our study highlights the effectiveness of tissue oxygenation and haemodynamic monitoring in this specific setting, caution is warranted when applying these results to other contexts. The inclusion of participants aged 60 or older undergoing elective off-pump CABG further limits applicability to younger patients or those undergoing other cardiac procedures.
Most cardiac surgeries involve cardiopulmonary bypass, which poses unique physiological challenges, including non-pulsatile flow, inflammation from blood contact with the circuit, and an increased risk of embolisation. These factors may enhance the utility of near-infrared spectroscopy as a monitoring tool in such settings.43 44 45 46 By contrast, off-pump CABG is characterised by haemodynamic fluctuations caused by manipulation of the beating heart,47 48 49 mimicking real-world perioperative challenges related to preload, afterload, and contractility changes.8 10 50 While the mechanisms underlying haemodynamic fluctuations differ across surgical contexts, off-pump CABG provides a valuable model for understanding and managing haemodynamic instability in diverse perioperative scenarios. Consequently, we postulate that our findings may be generalisable to populations receiving non-cardiac surgery where cardiopulmonary bypass is not utilised.
The 30 day follow-up period, while informative, may not capture long term effects, which will be evaluated in future analyses. Tissue oximetry provides an estimate of brain and muscle oxygenation that is well validated and widely accepted.20 51 The protocol followed a pragmatic approach, establishing specific oxygenation goals without mandating rigid interventions. Instead, we used a bundle of actions guided by physiological rationale, clinical judgement, available resources, and the underlying causes of oxygenation changes (fig 1). While the target goals of maintaining multisite tissue oxygenation close to baseline levels were achieved, outcomes might differ if alternative management strategies, such as varying ratios of fluids, vasopressors, or inotropes, were applied.
Finally, the adjustment for baseline imbalances, although prespecified in the statistical analysis plan, carries a risk of bias if the imbalances occurred randomly.52 53 Additionally, sparse event rates for secondary outcomes, such as stroke, introduce the potential for small sample bias, which could inflate risk ratios and should be interpreted with caution in this context.35
Conclusions
The Bottomline-CS trial tested whether perioperative care guided by multisite tissue oxygen saturation and facilitated by haemodynamic monitoring reduces complications after off-pump CABG. While guided management significantly improved intraoperative tissue oxygenation, no benefit was conferred for the primary composite of major complications, its individual components, atrial fibrillation, or hospital stay duration. The narrow confidence interval for the primary composite relative risk (width of 0.18) underscores the robustness of these neutral findings, ruling out insufficient power as an explanation. We conclude that integrating multisite tissue oxygenation into existing perioperative care protocols does not provide additional benefits in patients having off-pump CABG.
What is already known on this topic
-
Postoperative complications are common after cardiac surgery and may result from inadequate tissue perfusion
-
The role of maintaining multisite tissue oxygen saturation using near-infrared spectroscopy (NIRS) and haemodynamic monitoring in off-pump coronary artery bypass grafting (CABG) remains uncertain
-
Previous trials focused solely on NIRS monitoring of a single tissue bed and were limited by small sample sizes, with the largest involving only 249 patients
What this study adds
-
Postoperative complications were comparable between patients receiving NIRS and haemodynamic monitoring-guided care and those receiving usual care in off-pump CABG
-
These findings do not support the routine use of NIRS and haemodynamic monitoring to maintain tissue oxygenation
-
Future research should prioritise well powered studies targeting specific outcomes, such as pneumonia, to enhance perioperative care
Ethics statements
Ethical approval
The study protocol was approved by the internal review board of Tianjin Chest Hospital (2021KY-008-001).
Data availability statement
The code used to analyse the data in the paper can be found in the supplemental files. The data underlying the findings in this paper are openly and publicly available and can be found here: (DOI: 10.5061/dryad.z34tmpgqz). If you encounter problems accessing the data, please contact the corresponding author.
Acknowledgments
We thank the following people who contributed to the trial: Dongmei Meng, Peng Sun, Ruifang Gao, Yi Ren, Hong Xu, Bingsha Zhao, Yunfei Li, Ying Zhang, Yuezi Song, Yidan Wang, Jiapeng Liu, Jianxu Er, Jianjian Yu, Tong Zhao, Yifei Shi, Xiaowei Yang, Hui Liu, Dangpei Kou, Wenzhi Tian, Long Zhan, Liang Liu, Wei Bian, Jing Sun, Songhua Wu, Jie Li, Chang Xie, Yaobang Bai, Daoyu Wang, Nan Jiang, Lianqun Wang, Wei Dong, Bo Fu, Junzhe Zhang (Tianjin Chest Hospital, Tianjin University) and He Jiao (Tianjin University). We thank the Yale ClinicalTrials.gov Team at Yale University, New Haven, CT, USA for assisting in trial registration and management at ClinicalTrials.gov throughout the trial period. We also extend our gratitude to Nonin Medical, Inc (Plymouth, MN, USA) for loaning the tissue oximetry equipment and to LiDCO, now part of Masimo (Irvine, CA, USA), for loaning the haemodynamic monitor necessary for the study. Our appreciation goes to the perioperative team, including surgeons, anaesthesiologists, intensivists, nurses, and staff at Tianjin Chest Hospital (Tianjin, China), for their unwavering support in making this study possible. Additionally, we thank Feng Dai, previously affiliated with Yale University School of Public Health, for his assistance in developing the trial protocol, particularly the statistical analysis plan. Lastly, we thank the institutional/departmental sources provided by Tianjin Chest Hospital affiliated with Tianjin University and the Department of Anaesthesia at Indiana University School of Medicine.
Footnotes
-
Contributors: JH, ZG, DIS, and LM conceived the study. JH, ZG, DIS, and LM designed the study. JH, WZ, ZW, TW, ZZ, MR, ZG, and LM conducted the study. JH, WZ and TW coordinated and supervised the study. ZZ and ZL conducted analyses. JH, ZZ, WZ, ZW, MR, DIS, ZG, ZL, and LM interpreted the results. JH, DIS, and LM wrote the first draft of the manuscript. DIS and LM critically revised the manuscript. ZG, DIS, and LM contributed equally to this work and should be considered as co-corresponding authors. All authors approved the final version. JH has full access to all data and is responsible for its integrity. ZZ and ZL are responsible for the accuracy of the data analysis. JH and LM are the guarantors. The corresponding authors attest that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
-
Funding: This work was supported by the Tianjin Science and Technology Project (No. 20JCZDJC00810; ZG). It was also supported by the Tianjin Key Laboratory of Cardiovascular Emergency and Critical Care. The funders had no role in considering the study design or in the collection, analysis, interpretation of data, writing of the report, or decision to submit the article for publication.
-
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the Tianjin Science and Technology Project and the Tianjin Key Laboratory of Cardiovascular Emergency and Critical Care; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
-
Transparency: The lead authors (JH and LM) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
-
Dissemination to participants and related patient and public communities: As the personal identifying information of participants has been removed from the study dataset, it is not possible to send the results of this study to participants. Findings will be shared with clinicians and patients through national and international conferences and press releases.
-
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.