Evaluating patients with chest pain in the emergency department
BMJ 2025; 388 doi: https://doi.org/10.1136/bmj.r136 (Published 28 March 2025) Cite this as: BMJ 2025;388:r136
- Fernanda Bellolio, professor of emergency medicine1,
- Michael Gottlieb, professor of emergency medicine2,
- Richard Body, professor of emergency medicine3,
- Martin P Than, honorary research professor4,
- Erik P Hess, professor of emergency medicine5
- 1Mayo Clinic, Minnesota, USA
- 2Rush University Medical Center, Illinois, USA
- 3The University of Manchester, Manchester, UK
- 4University of Otago, Christchurch, New Zealand
- 5Vanderbilt University, Tennessee, USA
- Correspondence to: E P Hess erik.hess{at}vumc.org
Abstract
Identifying patients with chest pain that is of cardiac origin is crucial owing to the high mortality and morbidity of cardiovascular diseases. History, electrocardiogram, and cardiac biomarkers are the core elements of the assessment. High sensitivity cardiac troponins (hs-cTn) are the preferred biomarkers for diagnosing acute myocardial infarction, allowing for more accurate detection and exclusion of myocardial injury. However, elevations in hs-cTn can occur in patients who are not experiencing acute myocardial infarction. Therefore, it is important for clinicians to recognize how to integrate hs-cTn levels into their clinical decision making process. Structured risk assessments, using evidence based diagnostic protocols, should be employed to estimate the risk of acute coronary syndrome and adverse events in patients with chest pain. Clinical decision pathways should be used routinely in emergency departments. Patients at intermediate or high risk of obstructive coronary artery disease might benefit from cardiac imaging and further testing. Patients should be involved in decision making, with information provided about risks, radiation exposure, costs, and alternative options to facilitate informed decision making.
Introduction
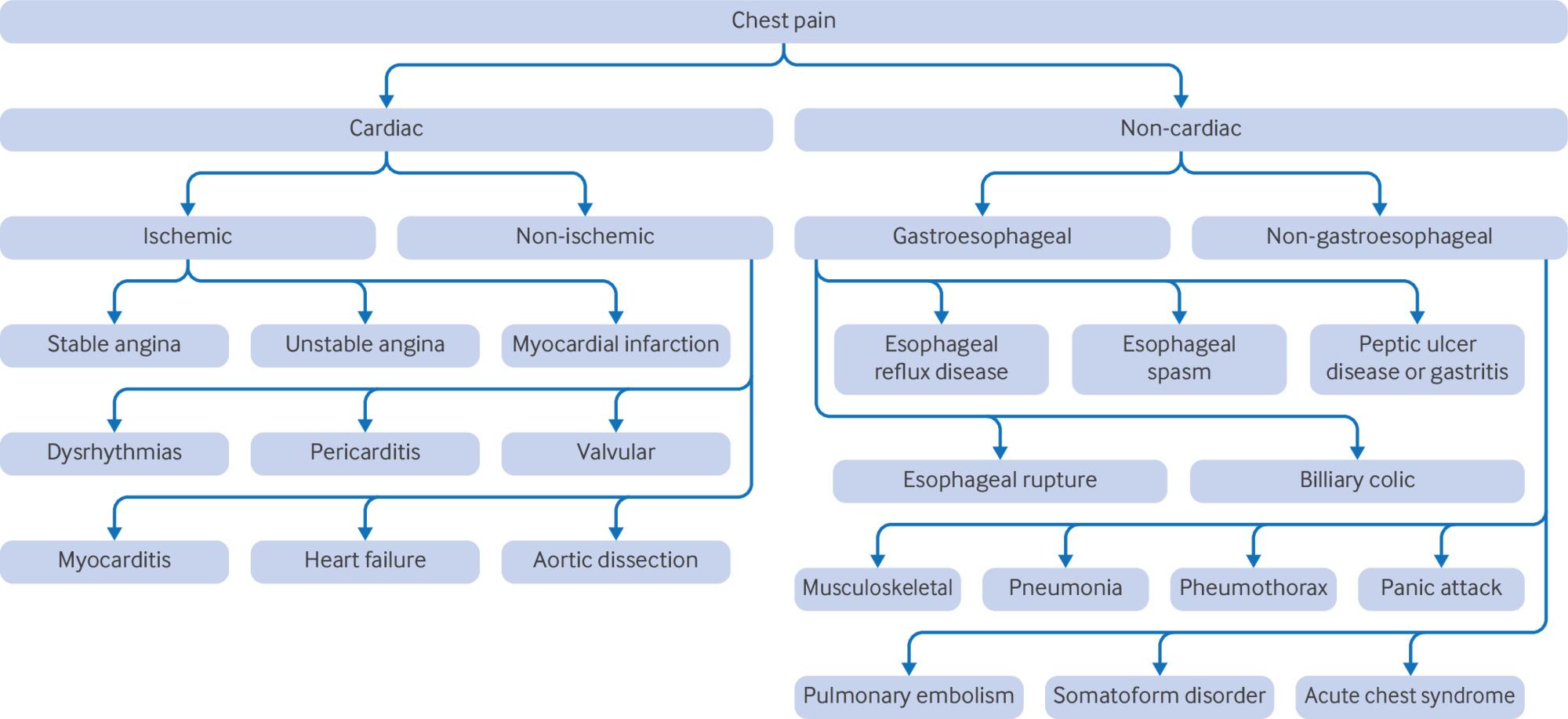
Chest pain is the second most common presenting symptom to the emergency department, accounting for nearly 5% of visits.1 Chest pain encompasses more than just discomfort in the chest; it includes pain, pressure, tightness, or discomfort in areas like the shoulders, arms, neck, back, upper abdomen, or jaw, as well as symptoms like shortness of breath and fatigue. Public awareness campaigns encourage people to seek medical assessment if they have chest pain or other symptoms of possible cardiac origin, because early identification or exclusion of life threatening causes is critical. The differential diagnosis for chest pain is broad and includes acute coronary syndrome (ACS), acute aortic syndromes, pericarditis, myocarditis, pulmonary embolism, pneumothorax, pneumonia, and peptic ulcer.
Coronary artery disease (CAD) is characterized by the presence of atherosclerotic plaques within the coronary arteries, which can lead to chronic stable angina or remain asymptomatic. Over time, these plaques can become unstable, leading to plaque rupture or erosion, which is the primary pathophysiological mechanism underlying ACS.2 CAD is a risk factor for ACS. CAD is defined in most trials as a history of myocardial injury or infarction, coronary revascularization, or ≥50% coronary stenosis.345
ACS is frequently caused by the rupture, fissure, or erosion of an atherosclerotic plaque resulting in intraluminal coronary thrombosis and downstream myocardial injury or infarction and represents a small percentage of all patients who present with chest pain.6 Given the high incidence of chest pain in the emergency department, the sizable risk associated with ACS, and the high prevalence of CAD, evaluating acute chest pain involves considerable clinical uncertainty, resource utilization, testing, and cost implications.
We provide an up to date review for clinicians evaluating patients with acute chest pain in the emergency department in whom ACS is the primary diagnostic consideration. We incorporate recent changes in algorithms secondary to the increased use of high sensitive cardiac troponin (hs-cTn), risk stratification tools that utilize hs-cTn, and discuss updates in the clinical guidelines.
Sources and selection criteria
A medical librarian performed five independent literature searches in the following databases: Medline, Embase and ClinicalTrials.gov. Search terms included “acute coronary syndrome” or “chest pain.” Other terms: emergency and (troponin, electrocardiography, electrocardiogram, ECG, EKG, risk, decision, path, imaging, or CT). We included studies from 1 January 2000 to 23 July 2024. Only articles in English were reviewed. After duplicates were removed, we screened 277 titles and abstracts for decision making, 1097 for ECG, 547 for imaging, 2746 for risk stratification, and 1174 for troponin. We evaluated studies based on the quality of study design, prioritizing randomized controlled trials over observational studies, relevance to the topic, and more recent publication dates. Although this was a comprehensive literature search, we did not design this manuscript as a systematic review. If existing systematic reviews were available and appropriate, these were utilized.
Epidemiology
Chest pain is a common presenting symptom in both emergency and outpatient settings, leading to 6.5-7.8 million emergency department visits annually in the United States (US).17 Of all patients who present with chest pain, only 5.1% will have ACS, and more than half will have a non-cardiac cause.1 Although the etiology of chest pain is often non-cardiac, CAD affects more than 20 million adults in the US and remains the leading cause of death (more than 606 000 deaths annually).8 Furthermore, recurrent emergency department visits for chest pain are common, with up to 40% of patients returning to the emergency department for chest pain within one year.9
The cost burden of acute chest pain is substantial, with estimated healthcare costs ranging from $13 000-$15 000 million for emergency department visits alone, and additional substantial costs associated with inpatient care and ACS management.1011 Every 40 seconds, one person will have a myocardial infarction, including 720 000 with a new coronary event and 335 000 with a recurrent event. The mean age at first myocardial infarction is 65.6 years for men and 72.0 years for women. Approximately 70% of these cases are non-ST-elevation myocardial infarction (NSTEMI) and unstable angina. These patients typically present with more comorbid conditions compared with those with ST-segment elevation myocardial infarction (STEMI). There is a higher prevalence of CAD in men compared with women.12 Sex differences in pathophysiology are notable, with women more likely to have non-obstructive CAD. Women are also less likely to receive coronary angiography, percutaneous coronary intervention, and guideline-directed medical therapy after acute myocardial infarction compared with men.113
A systematic review of 181 studies conducted primarily in high income countries found that lower socioeconomic status (education, income, insurance, occupation, or a composite) was associated with a higher incidence of ACS (incidence rate ratio, 1.1-4.7), a higher prevalence of ACS (odds ratio, 1.8-3.9), a higher odds of receiving suboptimal medical care (odds ratio, 1.1-10.0), and higher mortality (hazard ratio, 1.10-4.13).14 An analysis conducted in the CARDIA study (Coronary Artery Risk Development in Young Adults; n=5112) with a median follow-up of >33 years identified that premature cardiovascular disease risk in black participants was attenuated after adjustment for lifestyle, neighborhood, and socioeconomic factors. For example, the 2.4-fold increased cardiovascular disease risk in black women relative to white women was no longer after adjusting for clinical, lifestyle, socioeconomic, and neighborhood factors. After adjusting for social determinants of health and cardiovascular risk factors, black men and women have similar risk for fatal CAD (1.00, 95% confidence interval 0.54 to 1.85) and lower risk for non-fatal CAD (0.70, 0.46 to 1.06) compared with white men and women.1215
Trends in non-invasive testing
Regarding the approach and evaluation of chest pain, recent trends of doing less invasive testing have been supported by studies like the secondary analysis of the Rule Out Myocardial Ischemia/Infarction by Computer Assisted Tomography (ROMICAT-II) trial from nine emergency departments in the US. Patients who underwent clinical evaluation alone had a shorter length of stay (20.3 v 27.9 hours; P<0.001), lower rates of angiography (2% v 11%; P<0.001), lower median costs ($2261 v $2584; P<0.01), and less radiation exposure (0 v 9.9 mSv; P<0.001) compared with those who underwent cardiac testing. Patients without cardiac testing also had lower rates of adverse cardiac events (0% v 9%; P<0.001), lower rates of coronary angiography and percutaneous coronary intervention (0% v 10%; P<0.001, and 0% v 4%; P=0.02, respectively) during the index visit. There was no difference in rates of percutaneous coronary intervention (2% v 5%; P=0.15), coronary artery bypass surgery (0% v 1%; P=0.61), return emergency department visits (5.8% v 2.8%; P=0.08), or main adverse cardiac events (2% v 1%; P=0.24) at 28 days. Patients with negative biomarkers who underwent imaging or functional stress testing had longer length of stay, more downstream testing, increased radiation exposure, and greater cost without an improvement in clinical outcomes.16 Similarly, in a claims analysis of 536 197 patients with acute chest pain and without initial findings of ischemia, cardiovascular testing was associated with an increase in coronary angiography (36.5 per 1000 patients tested) and revascularization (22.8 per 1000 patients tested) at one year, but no change in myocardial infarction admissions (7.8 per 1000 patients tested).17 Another claims based study of 2 047 799 emergency department patients with chest pain who had a computed tomography coronary angiogram performed was associated with higher rates of percutaneous coronary intervention, coronary artery bypass surgery, repeat non-invasive testing, hospitalization, and return visits to the emergency department.18
Clinical assessment and risk stratification
Initial evaluation
Obtain a detailed history and focused physical examination. This should include the history of the present illness, including pain characteristics, duration, risk factors, and associated symptoms. Chest pain should not be described as atypical, because this descriptor is not helpful in determining the cause and implies a benign etiology. Figure 1 shows the differential diagnosis.

{kind=link}
A focused physical examination is also important. Assess the patient’s vital signs, perform a heart and lung examination, and note any signs of distress such as tachypnea, diaphoresis, or mottled skin. Likelihood ratios are used to assess the value of a diagnostic test and to help determine how a test result (positive or present and negative or absent) will change the probability of having a disease. Prior abnormal stress test, peripheral artery disease, CAD, pain radiating to both arms, and pain like prior episodes of ischemia are associated with ACS (table 1).192021222324
Probability of history and physical exam findings in acute coronary syndrome
Immediate evaluation
Electrocardiogram
The first step in the evaluation of patients with symptoms concerning for ACS is a 12 lead electrocardiogram. Guidelines recommend that the first electrocardiogram be obtained within 10 minutes of presentation.1 Promptly assess the electrocardiogram for findings diagnostic of ST-segment elevation myocardial infarction (STEMI) (fig 2), non-ST-segment elevation ACS (NSTE-ACS), hyperacute T waves, pericarditis, or a cardiac dysrhythmia.25 If the initial electrocardiogram is non-diagnostic but the patient continues to experience symptoms suggestive of ACS, repeat the electrocardiogram because ACS is a dynamic process. Also, assess the electrocardiogram for findings of alternate etiologies (see supplementary table).

ST-segment elevation myocardial infarction includes new ST-segment elevation at the J point in two contiguous leads ≥1 mm in all leads other than V2-V3, where the following cut-points apply: ≥2 mm in men ≥40 years; ≥2.5 mm in men <40 years, or ≥1.5 mm in women regardless of age
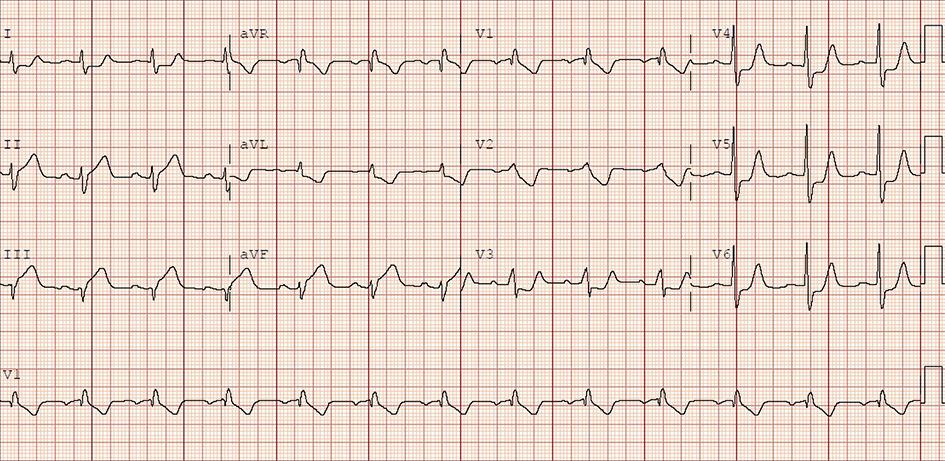{kind=link}
The presence of ST-segment elevation, a new left bundle branch block, or dynamic ST-segment changes (fig 3) is suggestive of acute myocardial infarction (AMI). In a systematic review assessing the diagnostic accuracy of STEMI criteria, the criteria were 43.6% sensitive and 96.5% specific for occlusion myocardial infarction.26 ST-segment elevation can also occur with diagnoses other than STEMI, such as pericarditis, early repolarization, hyperkalemia, hypercalcemia, Takotsubo cardiomyopathy, and left ventricular aneurysm.27

ST-segment depression with new horizontal or down sloping ST-segment depression ≥0.5 mm in two contiguous leads or T wave inversion >1 mm in two contiguous leads with prominent R wave or R/S ratio >1
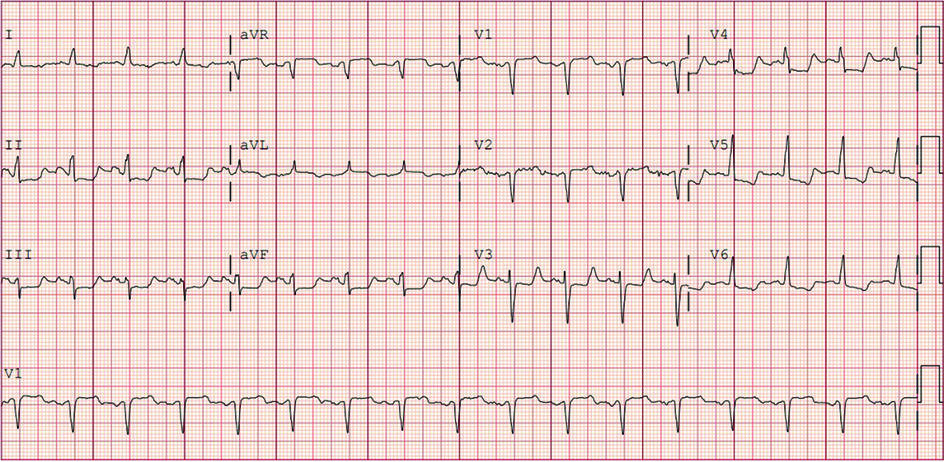{kind=link}
Overall, less than half of patients with suspected ACS and left bundle branch block are ultimately diagnosed with AMI.28 To increase the diagnostic accuracy for occlusion myocardial infarction in the setting of a left bundle branch block or a paced rhythm, additional electrocardiogram criteria have been developed (table 2).2930 The modified Sgarbossa criteria are the most accurate.31
High sensitivity cardiac troponins (hs-cTn)
Testing for cardiac troponin (cTn) is a cornerstone of the diagnostic approach.1 Troponin is a protein contained within the myofibrillar apparatus that is found in both skeletal and cardiac muscle. It is possible to test for the cardiac isoforms of both troponin I (cTnI) and troponin T (cTnT) with high analytical specificity. Early cTn assays were developed in the 1980s, but sensitivity and precision have improved.32 Widespread adoption of hs-cTn testing has enabled the development of rapid rule out pathways that can identify patients with a very low probability of AMI within a few hours of emergency department arrival.
The principal difference between this generation of hs-cTn and previous cTn assays is that, although they use similar technological methods, the high sensitivity assays can detect much lower blood concentrations of troponin and can do so with greater precision.3334353637Box 1 shows the technical terminology used concerning troponin assays. Table 3 shows the wide confidence margins for assay 99th percentiles. Clinicians often use the 99th percentile in a dichotomous manner to categorize results as positive or negative. Troponin is a continuous variable and, thus, indiscriminate use of cut-off points like the 99th percentile is not recommended. The 99th percentiles determined by manufacturers for their assays have an assigned imprecision. This is caused by several effects such as inconsistent criteria for reference populations; technical problems with assay manufacturing leading to variation between production lots; variation due to sex, ethnicity, and geography; and small sample sizes of the reference populations used.
Troponin definitions and ranges38
Coefficient of variation (CV)—A statistical term for assay consistency that describes the reproducibility of a result at a given level if the sample were to be tested over and over again.
Limit of blank (LOB)—The highest apparent analyte concentration expected to be found when replicates of a blank sample containing no analyte are tested (ie, it is possible to get this result even if no troponin is present).
Limit of detection (LOD)—The minimum concentration of troponin at which a troponin can reliably be considered to have been detected. The LOD is always higher than the LOB.
Limit of quantification (LOQ)—The minimum concentration at which the CV is ≤20%. It is always higher than the LOD. Because precision at the LOD can be poor but precision at the LOQ is fixed (eg, a CV of ≥20%), some jurisdictions (eg, the US Federal Drug Administration rules) do not allow reporting of troponin results below the LOQ.
99th Percentile and upper reference limit (URL)—Represents a cut-off point below which 99% of the results occurred in a reference healthy population. Levels recorded above this (Upper Reference Limit or URL) are considered to be abnormal.
hs-cTn—High sensitive cardiac troponin.
Detectable non-elevated hs-cTn—Values ofhs-cTn above the LOQ but below the 99th percentile URL.
Relative change (Δ) in hs-cTn—The percentage change in hs-cTn across serial measurements. Relative changes ≥20% may be indicative of acute myocardial injury. Change corresponding to more than 50% of the reference interval is a significant biological change. At low troponin concentrations near the 99th percentile URL, absolute Δ values provide greater specificity for acute myocardial injury than relative Δ values,.
Absolute change (Δ) in hs-cTn—The change in hs-cTn across serial measurements, reported as an absolute value in ng/L. At low hs-cTn concentrations near and below the 99th percentile URL use absolute Δ values, not relative Δ values. It is recommended that clinical decision pathways for discharge should use absolute Δ values, not relative Δ values.
Overall and sex specific 99th percentile upper reference limits for some current high sensitivity troponin assays39
In a meta-analysis of 17 studies and 8644 patients, baseline hs-cTn versus baseline cTn demonstrated better sensitivity (0.884 v 0.749; P<0.001) and negative predictive value (0.964 v 0.935; P<0.001), but lower specificity (0.816 v 0.938; P<0.001) and positive predictive value (0.558 v 0.759; P<0.001).40 The negative predictive value can be further improved to 99.1% to 100% with the use of serial troponins.41 In a study evaluating four strategies by using hs-cTnI to compare the limit of detection, single cutoff, 1 hour algorithm, and 0/1 hour algorithm, among 2828 patients, 16% had myocardial infarction. The limit of detection method ruled out 16% of patients with 100% sensitivity, and the single cutoff ruled out 54% with 97.1% sensitivity. The 1 hour and 0/1 hour algorithms ruled out about 52% with 98.4% sensitivity. For patients presenting within 2 hours of symptoms, the single cutoff had lower sensitivity (94.2%). Overall, all methods were effective, but the single cutoff was less suitable for patients who presented early.42 A systematic review of 32 studies and 30 066 patients evaluating the diagnostic accuracy of different hs-cTn timing strategies demonstrated that diagnostic performance was similar across the hs-cTnT (Elecsys; Roche), hs-cTnI (Architect; Abbott), and hs-cTnI (Centaur/Atellica; Siemens) assays.43
Consequences of the adoption of high sensitivity troponins
The ability to detect lower concentrations of troponin with greater precision has allowed for the development of modern clinical decision pathways with higher negative predictive value and earlier timeframes for troponin testing (often allowing serial troponins to be completed within 1-2 hours of arrival).44454647 Additionally, most guidelines now advocate for the use of a single troponin risk stratification approach for certain low risk patient groups who then might be suitable for early discharge from the emergency department.35
The ability of hs-cTn to precisely detect troponin concentrations means that a subset could include those without coronary ischemia.48 Clinicians must therefore have a good understanding of the test when interpreting the results. Because of their higher sensitivity, concentrations measured by using hs-cTn assays are often elevated compared with the older troponin assays for patients with systemic illnesses that cause increased myocardial demand. It is important to note that cardiac troponin concentrations will rise with any myocardial injury. It is therefore not a marker specific to AMI, and there are other causes of myocardial injury (box 2). Since patient management is determined by the cause of the elevation, it is important to understand the cause. Examples on how to rule out some of these conditions include imaging like computed tomography coronary angiogram (coronary artery dissection), laboratory blood work (anemia, heart failure, chronic kidney disease), echocardiogram (heart failure), magnetic resonance imaging (cardiomyopathy), cardiac catheterization (takotsubo cardiomyopathy), electrocardiogram, and cardiac monitoring (tachyarrhythmias, ventricular hypertrophy).
Reasons for elevated cardiac troponin values due to myocardial injury
Related to acute myocardial ischemia
Atherosclerotic plaque disruption with thrombosis
Related to acute myocardial ischemia due to imbalance of oxygen supply or demand
Reduced myocardial perfusion:
Coronary artery spasm, microvascular dysfunction
Coronary embolism
Coronary artery dissection
Sustained bradyarrhythmia
Hypotension or shock
Respiratory failure
Severe anemia
Increased myocardial oxygen demand
Sustained tachyarrhythmia
Severe hypertension with or without left ventricular hypertrophy
Other causes
Cardiac conditions
Heart failure
Myocarditis
Cardiomyopathy (any type)
Takotsubo cardiomyopathy
Coronary revascularization procedure
Cardiac procedure other than revascularization
Catheter ablation
Defibrillator shocks
Cardiac contusion
Systemic conditions
Sepsis, infectious disease
Chronic kidney disease
Stroke, subarachnoid hemorrhage
Pulmonary embolism, pulmonary hypertension
Infiltrative diseases (eg, amyloidosis, sarcoidosis)
Chemotherapeutic agents
Patients that are critically ill
Strenuous exercise
False troponin results
Falsely abnormal results can occur during analysis. Analytical causes of falsely abnormal results include rheumatoid factor, fibrin interference, hemolysis, autoantibodies, macro troponin and heterophile antibodies.49 Results can also be affected by high bilirubin and lipid levels and biotin. Additionally, spurious results from laboratory errors can occur with all assays resulting in unexpected high flier results. The technicalities of such interferences and abnormalities are beyond the scope of this review. However, their existence further emphasizes the need for careful incorporation of the clinical picture of the patient when interpreting troponin results. When a result appears inconsistent with clinical circumstances, this should be discussed with the local laboratory that might repeat the test with careful attention to processing or be able to look for interference. In addition, clinicians should consider measuring troponin concentrations by using an alternate assay.5051
Interpreting hs-cTn concentrations
The cardiologist Robert Jesse said that “when troponin was a lousy assay it was a great test, but now that it’s becoming a great assay, it’s getting to be a lousy test.”52 This means that with older, less precise assays that could not detect low concentrations, it was fairly certain that myocardial injury was caused by a coronary related problem when the troponin concentration was raised above the upper reference limit for the older assay. Hs-cTn assays provide highly precise information across a much broader quantitative range.
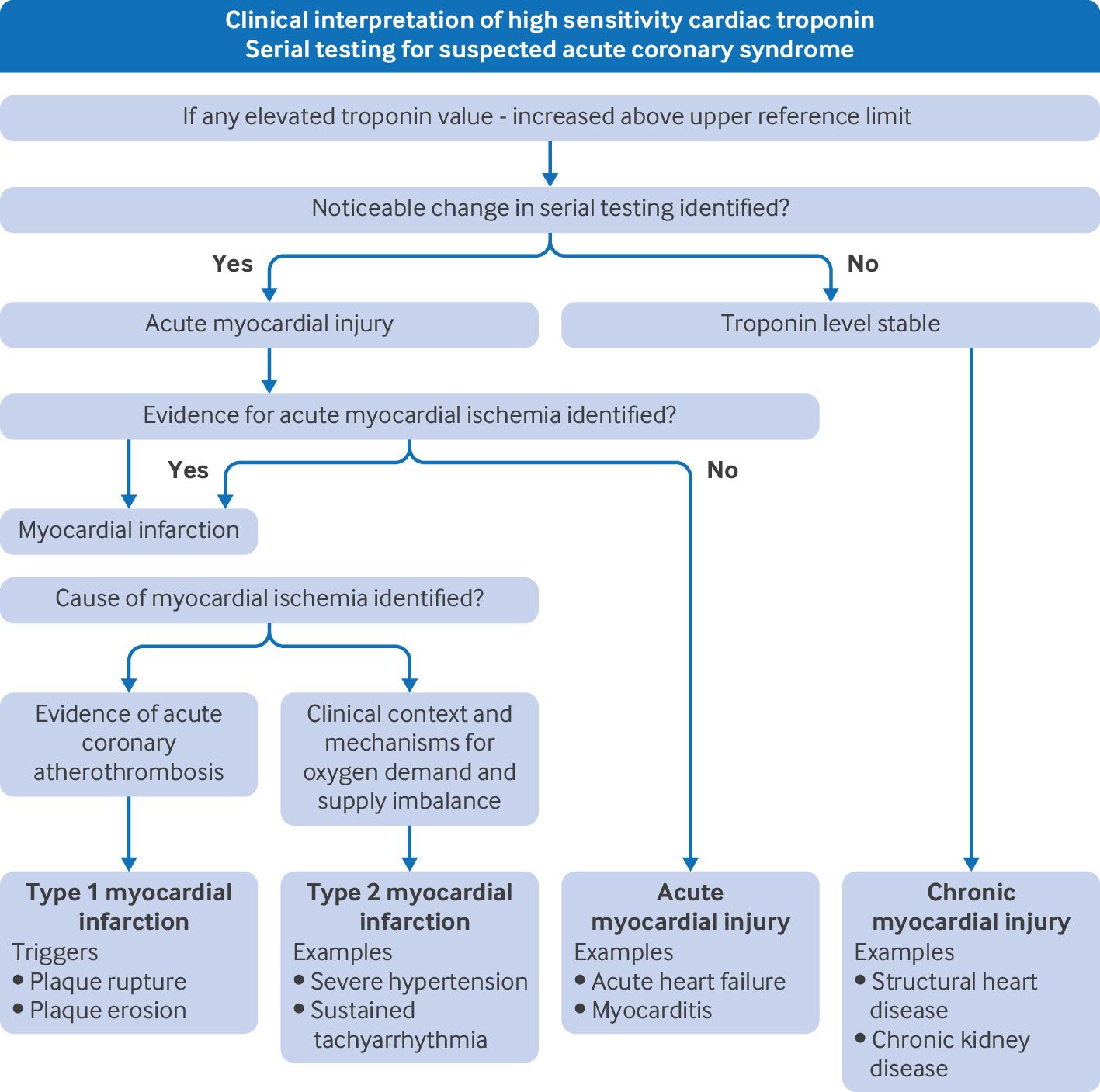
Raised concentrations of hs-cTn can be caused by the following:
Type 1 myocardial infarction
Type 2 myocardial infarction
Acute myocardial injury
Chronic myocardial injury
These distinctions are set out in the 4th Universal Definition of Myocardial Infarction.48Figure 4 shows a flow diagram for the interpretation of high sensitivity cardiac troponin.

Algorithm for clinical interpretation of high sensitivity cardiac troponin
{kind=link}
Clinical medicine has historically focused on detecting and managing patients classified here as type 1 AMI. However, patients with type 2 AMI, acute myocardial injury, and chronic myocardial injury also have high 5 year event rates.53 In particular, patients with type 2 AMI have high rates of undiscovered and untreated coronary and structural heart disease. In the DEMAND-MI study (Determining the Mechanism of Myocardial Injury and Role of Coronary Disease in Type 2 Myocardial Infarction), a cohort of patients categorized as type 2 AMI underwent investigation for structural heart disease and CAD. Some degree of CAD was found in 68% of patients, with obstructive disease in 30%. A large proportion of these patients were not receiving treatment with either anti-platelet drugs or statins. Similarly, 34% of patients had undiscovered structural heart disease (19% with severe disease), with notable gaps in therapy.54 Such patients are often admitted to general medicine teams (rather than cardiology) and are less likely to receive follow-up investigations or medications.
Another common group is patients with kidney disease. In a study of 15 111 patients presenting to seven emergency departments in Sweden, one third of patients with acute kidney injury had hs-cTnT concentrations indicative of acute myocardial injury without evidence of myocardial injury or infarction decreasing the specificity of hs-cTnT compared with patients without acute renal impairment.55 Implications of troponin concentrations near the 99th percentile are presented in box 3.
Implications of troponin concentrations below but near the 99th percentile
Troponin concentrations that are below the 99th percentile when measured by a high sensitivity assay are frequently described as normal or false negative. However, such dichotomization of a continuous variable has limitations. Patients presenting with chest pain who have troponin concentrations in the upper half of the range between the limit of detection and the 99th percentile (we will describe them here as high normals) have higher cardiac event and death rates in medium to long term follow-up. These patients warrant additional scrutiny regarding the potential need for follow-up investigations and consideration for secondary prevention medications such as statins.
In a Swedish study of 22 589 patients aged over 25 presenting to the emergency department with chest pain, 55 patients were followed for all cause mortality for approximately five years. Death in patients whose hs-cTnT result was <5 ng/L died of predominantly non-cardiac causes (top five were lung, breast, prostate, and colon cancer, and other unspecified causes). However, patients with nominally normal (but higher concentrations between 10-14 ng/L) died of predominantly cardiovascular causes (AMI, atherosclerotic cardiovascular disease, hemorrhagic stroke, and heart failure in addition to lung cancer). Mortality in the 10-14 ng/L group of patients was 15%, with notable rates of cardiovascular mortality (3.4%), AMI (3.9%), and heart failure (5.0%).
RETURN TO TEXTChest radiography
Although chest radiography is frequently obtained when evaluating patients with chest pain, findings infrequently lead to intervention, and their use should be guided by clinical suspicion.5657 In patients with chest pain and dyspnea, a chest radiograph can identify signs of fluid overload such as pulmonary vascular congestion and edema. A chest radiograph can also identify other acute cardiopulmonary causes of chest pain such as aortic dissection, pneumonia, or pneumothorax. The use of chest x ray has been recommended by the 2022 American College of Cardiology (ACC) Expert Consensus Decision Pathway and by the American College of Radiology (ACR). Although chest x ray is not sufficient to confirm or exclude CAD, it can demonstrate clinically important pathology in a meaningful minority of patients suspected to have ACS.1138
Point of care ultrasound
In a patient with acute chest pain and a non-diagnostic initial electrocardiogram, point of care ultrasound can identify regional wall motion abnormalities suggestive of ACS. However, accurate identification of regional wall motion abnormalities and differentiating acute from chronic abnormalities requires substantial expertise and should be assessed by more advanced users of echocardiography.58 Point of care ultrasound can also help rapidly identify pulmonary edema and has been shown to be helpful in the diagnosis of acute dyspnea in the emergency department.59
Cardiac testing
There are two main types of non-invasive advanced cardiac testing: anatomic and functional (box 4). Anatomic testing like computed tomography coronary angiogram directly visualizes the coronary arteries and can estimate the degree of coronary stenosis. Though estimates of fractional flow reserve and thus functional cardiac information can be obtained from computed tomography coronary angiogram, these estimates are not widely available in most centers.61 A systematic review on the effectiveness of computed tomography coronary angiogram in patients with acute chest pain (22 studies, 9379 participants) demonstrated a similar incidence of AMI (relative risk 0.86; 95% confidence interval 0.66 to 1.12), all cause mortality (0.96; 0.59 to 1.58), and cardiovascular mortality (1.35; 0.59 to 3.09) compared with usual care, irrespective of pretest probability.62 In patients at low to intermediate risk of ACS (as defined by a risk score), there were more revascularizations (1.45; 1.09 to 1.93) and medication changes (1.33; 1.06 to 1.67). There was increased radiation exposure (mean difference 7.24 mSv; 95% confidence interval 4.55 to 9.94) for patients who had a computed tomography coronary angiogram. Computed tomography coronary angiogram for patients at low to intermediate risk for ACS was associated with a 17% reduction in length of stay in hospital and a 21% decrease in immediate costs.62
Common anatomical and functional testing options13860
1. Coronary computed tomography angiography (CCTA or CTCA) is a non-invasive imaging modality that provides detailed images of the coronary arteries. It is particularly useful for ruling out coronary artery disease (CAD) in patients with low to intermediate risk of acute coronary syndrome (ACS). CTCA can detect both non-obstructive and obstructive plaque and can identify non-cardiac causes for some symptoms.
2. Stress echocardiography has excellent accuracy, sensitivity and specificity. It provides additional information on wall thickness, chamber size, and valvular abnormalities, without radiation or contrast dye.
3. Stress cardiac magnetic resonance (CMR) is another non-invasive imaging technique that can assess myocardial perfusion and viability. Stress CMR is often used in patients with known CAD and/or cardiomyopathy, and it is contraindicated in patients with major renal dysfunction.
4. Stress/rest single photon emission computed tomography (SPECT) myocardial perfusion imaging is widely available and has relatively high diagnostic sensitivity. It is used to assess ventricular function and detect perfusion abnormalities. SPECT is preferred in patients who cannot exercise or who have severe bronchospastic disease.
5. Stress/rest positron emission tomography (PET) myocardial perfusion imaging offers high diagnostic accuracy and lower radiation exposure compared with SPECT. It can measure myocardial blood flow and flow reserve. PET is preferred over SPECT owing to its higher diagnostic accuracy and lower rate of non-diagnostic test results.
RETURN TO TEXTOther types of cardiac testing (exercise electrocardiogram, stress/rest single photon emission computed tomography myocardial perfusion imaging, stress/rest stress echocardiography, and stress/rest positron emission tomography) provide information on cardiac function. Current guidelines recommend selective use of testing, reduced layered testing, and eliminating testing when the diagnostic yield is low. Resting imaging tests, including radionuclide myocardial perfusion imaging and echocardiography, could be of value in the evaluation of patients who have persistent chest pain suggestive of ACS, a non-ischemic electrocardiogram, and initial or serially negative cardiac biomarkers. Some patients in whom chest pain has resolved might undergo stress testing with or without imaging in the outpatient setting. Stress echocardiography shows excellent accuracy compared with coronary angiography for detecting CAD, with similar sensitivity to nuclear perfusion imaging but with higher specificity. It also provides additional information on wall thickness, chamber size, and valvular abnormalities, without radiation or contrast dye.63
A systematic review of 34 studies (3352 participants) found exercise testing for CAD varies in accuracy based on age, sex, and test type. Treadmill echocardiography (likelihood ratio 7.9), treadmill electrocardiogram (3.6), and bicycle echo (11.3) had the highest positive likelihood ratios. Exercise tests are better at ruling out CAD than confirming it, especially in younger patients (4.7).64 A systematic review including 77 studies demonstrated that negative computed tomography coronary angiogram has a higher test performance than other index tests to exclude clinically important CAD. A positive stress myocardial computed tomography perfusion added to computed tomography coronary angiogram, stress cardiac magnetic resonance, and positron emission tomography have a higher test performance to identify patients requiring invasive coronary artery evaluation.65 A study including 15 000 patients with a pooled prevalence of CAD of 14.9%, showed that the greatest ruling out capacity (ie, post-test probability <5%) was by computed tomography coronary angiogram, positron emission tomography, and stress cardiac magnetic resonance. With decreasing pre-test probability, the number of false positive tests increased.66 A study of 5332 patients showed a sensitivity of computed tomography angiography of 95.2% and specificity of 79.2%. At a pretest probability of 7%, the positive predictive value of computed tomography angiography was 50.9% and the negative predictive value was 97.8%; corresponding values at a pretest probability of 67% were 82.7% and 85.0%, respectively. Performance of computed tomography angiography was not affected by the type of chest pain and was slightly higher in men and lower in older patients.6768
The warranty period of prior cardiac testing should be considered when symptoms are unchanged. A normal coronary angiogram with no stenosis or plaque warranty period is two years, and a normal stress test warranty period, given adequate stress, is one year.19Table 4 outlines considerations in stress testing selection and contraindications to testing. The primary considerations are whether the patient can exercise and whether imaging is needed. Other considerations include resting electrocardiogram, additional information provided by the test, test availability, radiation exposure, and cost.
Stress testing selection and contraindications63
Risk scores and risk stratification
Pathways and risk scores are integral to the efficient and accurate evaluation of chest pain in the emergency department, ensuring that patients receive appropriate care that is based on their risk level.386970
Risk scores for possible ACS
Several risk scores have been evaluated. Some that were derived for prognostication in patients with established ACS were initially repurposed so that they could be used in the emergency department setting. The Thrombolysis in Myocardial Infarction score, which uses a simple six point scale, is one example. Recently, more risk scores have been developed specifically for risk stratification of undifferentiated emergency department patients with suspected ACS. The history, electrocardiogram, age, risk factors, and troponin (HEART) score was developed based on clinician intuition and uses the degree of clinical suspicion based on symptoms, electrocardiogram, age, CAD risk factors and troponin concentrations. Additional risk scores have been derived and validated using multivariable analyses to identify independent predictors of AMI and major adverse cardiac events. These include the Emergency Department Assessment of Chest Pain Score and the Troponin-only Manchester Acute Coronary Syndromes score.37717273
The thrombolysis in acute myocardial infarction score and HEART score have been applied both with a single hs-cTn test at the time of arrival in the emergency department and with serial hs-cTn testing over 1-3 hours.374 The Emergency Department Assessment of Chest Pain Score (EDACS) score was designed to be used with serial troponin testing over 2 hours,74 while the Troponin-only Manchester Acute Coronary Syndromes score was designed for use with a single hs-cTn test at the time of arrival.367576
Compared with an unstructured clinical assessment, risk scores have been shown to decrease unnecessary testing and reduce admissions while maintaining high sensitivity for the detection of acute myocardial injury and 30 day major adverse cardiac events.12377 Major adverse cardiac events usually incorporate cardiac death, AMI occurring after discharge from the emergency department, and coronary revascularization. Coronary revascularization is more controversial as an outcome measure to drive practice given the potential for variation in practice and a lack of data to support the effectiveness of urgent coronary revascularization when AMI has been ruled out.
Table 5 summarizes the systematic reviews that evaluate the diagnostic accuracy and efficiency of each of these risk scores.
Risk stratification tools for suspected acute coronary syndrome
hs-cTn=high-sensitivity cardiac troponin; MACE=major adverse cardiac events
Machine learning techniques allow us to consider hs-cTn as a continuous variable rather than imposing a cutoff, as with the Troponin-only Manchester Acute Coronary Syndromes score. There are advantages to this approach, because a very high hs-cTn concentration is likely to be more concerning than a slightly raised value. For example, the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome model was derived in a dataset of 10 038 patients, and on external validation in 10 286 patients from seven cohort studies, the model had an area under the receiver operating characteristic curve of 0.953.83 Further, the Myocardial Ischemic Injury Index model can provide important practical support in the interpretation of serial hs-cTn results. This model considers age, sex, hs-cTn results and their timing to determine whether an observed change in hs-cTn concentration on serial sampling is meaningful. The model had an area under the receiver operating characteristic curve of 0.949 when it was validated in 20 761 patients. This could have practical value in busy emergency departments when precise timing of serial sampling at 1 h, 2 h, or 3 h is not feasible.84
In direct comparisons, the thrombolysis in acute myocardial infarction has been outperformed by HEART, Troponin-only Manchester Acute Coronary Syndromes score and Emergency Department Assessment of Chest Pain Score for diagnostic efficiency and sensitivity for AMI and major adverse cardiac events.75828586 Troponin-only Manchester Acute Coronary Syndromes score had higher sensitivity for AMI and major adverse cardiac events than both HEART and Emergency Department Assessment of Chest Pain Score,82 though Emergency Department Assessment of Chest Pain Score has been shown to have similar sensitivity outside of North America.75
Clinical decision pathways
Whether used alone or with a risk score, hs-cTn testing must guide clinical decision making in the emergency department. This requires incorporating hs-cTn into a clinical decision pathway. Numerous pathways have been developed. As a general principle, decision pathways will specify criteria to rule out AMI after performing single hs-cTn test at the time of arrival in the emergency department. After considering alternative diagnoses and other relevant factors, such patients might be eligible for early discharge. Patients with a hs-cTn level above a very high threshold have a high probability of AMI, and the diagnosis could be considered ruled in, allowing for early specialist referral and treatment. The remaining patients will undergo a second hs-cTn test one to three hours after the first test. This will stratify more patients to the rule out and rule in groups. The remaining patients could be in an observation group. The European Society of Cardiology recommends a decision pathway that uses serial hs-cTn testing over 1 hour.87 The cutoffs and delta criteria (the change between hs-cTn levels on serial samples) are separately derived for each commercially available hs-cTn assay. In the UK, the National Institute for Health and Care Excellence (NICE) commissioned a systematic review which identified numerous hs-cTn testing pathways with high sensitivity, with the choice of any particular decision pathway being deferred to individual hospitals based on local factors.88 For example, laboratory turnaround times and emergency department crowding might make serial sampling after 1 hour logistically challenging. A hospital might defer the second test, when required, for two or even three hours. Implementation of clinical pathways for suspected ACS reduced the length of stay and increased the proportions of patients safely discharged within six hours.89
Risk scores can also be used to guide decision pathways. Troponin-only Manchester Acute Coronary Syndromes score stratifies patients into four risk groups based on the calculated probability of ACS after a single hs-cTn test. Each risk group has a recommended disposition. The HEART pathway requires the use of the HEART score to stratify patients into low, moderate, and high risk groups. The low risk group is eligible for discharge after two hs-cTn tests performed three hours apart. In a randomized trial, this pathway reduced objective testing and increased early discharges.3
A multicenter study with 17 384 patients showed that the use of hs-cTn improved the detection of myocardial infarction in the emergency department (4.6% v 2.0%; P<0.001) and within 30 days (5.8% v 4.4%; P<0.001) compared with non-hs-cTn testing. The 30 day all-cause mortality rate was unchanged (0.3% v 0.4%; P=0.50). Also, patients in the hs-cTn group had lower healthcare use (admission rate 12.2% v 15.0%, stress testing 10.2% v 12.8%, and revascularization 1.0% v 2.0%; P<0.001 for all).90 However, the High-Sensitivity Troponin in the Evaluation of patients with Acute Coronary Syndrome pathway, which requires serial hs-cTn testing over three hours without a risk score, has been reported to have greater diagnostic efficiency than HEART without compromising sensitivity.53
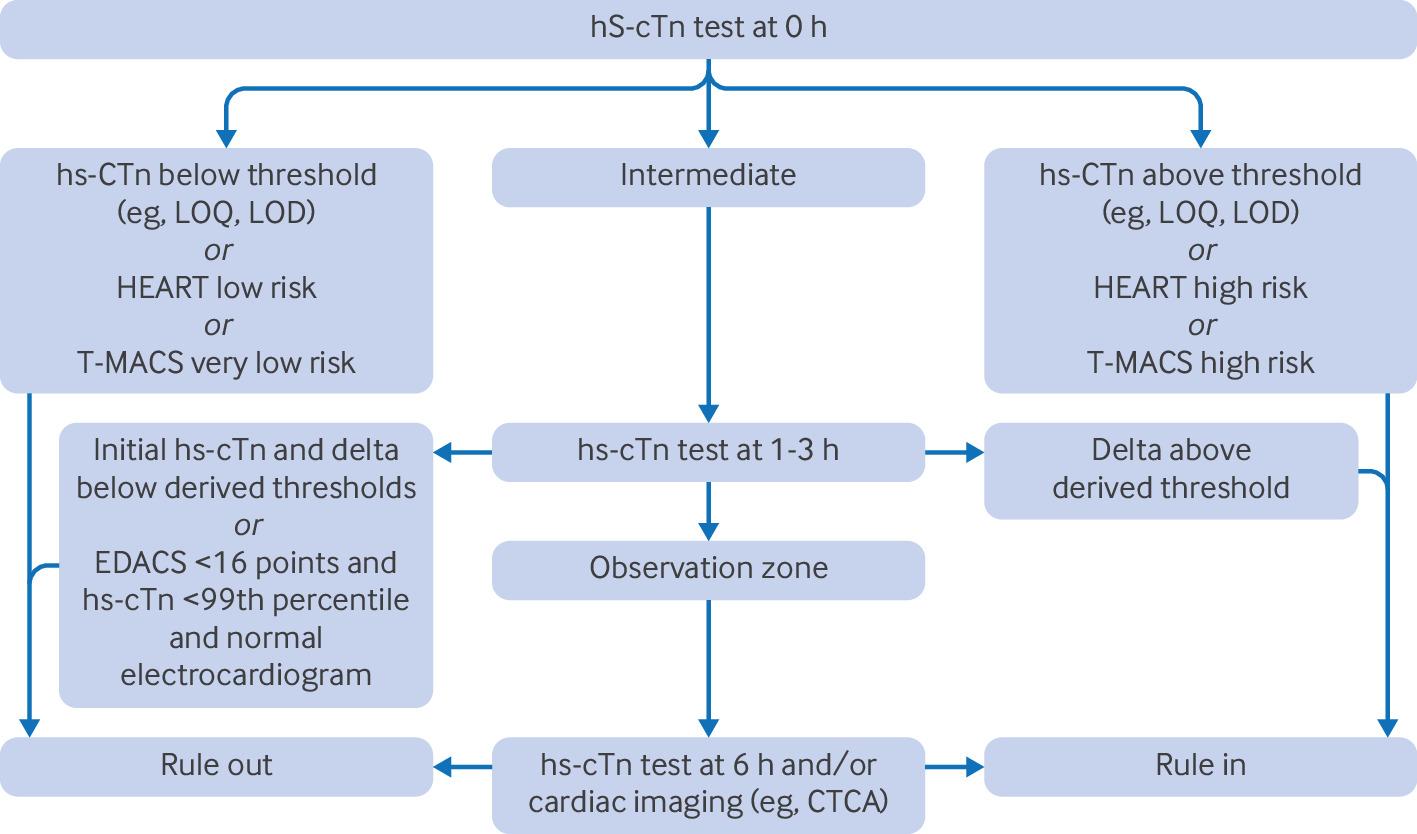
A key unanswered question in this field is the optimum management of patients in the observation group. Given the intermediate probability of AMI, a reasonable initial approach is to repeat the hs-cTn test at six hours to confirm or refute the diagnosis with greater certainty. Imaging, such as computed tomography coronary angiogram, could then be considered for the remaining patients who do not have AMI. Figure 5 shows a rubric for a clinical decision pathway for patients with suspected ACS, with or without the use of risk scores.

Clinical decision pathways for patients with suspected acute coronary syndrome. LOQ=limit of quantitation; LOD=limit of detection; HEART=history, electrocardiogram, age, risk factors, and troponin; T-MACS=Troponin-only Manchester Acute Coronary Syndromes; EDACS=Emergency Department Assessment of Chest Pain Score (EDACS); CTCA=computed tomography coronary angiogram
{kind=link}
Does the addition of a risk score to hs-cTn help identify patients safe for emergency department discharge?
The incremental value of risk scores in the era of hs-cTn is debated. A systematic review of risk stratification scores included six external validation studies and 20 959 patients.91 A HEART score ≤3 predicted a very low risk of major adverse cardiac events among the greatest proportion of patients. Other scores (thrombolysis in acute myocardial infarction, Global Registry of Acute Coronary Events, No Objective Testing Rule, Emergency Department Assessment of Chest Pain Score) had lower sensitivity or classified fewer patients as low risk. Overall, the HEART score effectively identified low risk patients, and the risk of major adverse cardiac events was so low that additional testing might not be necessary. The Sensitivity Troponin in the Evaluation of patients with Acute Coronary Syndrome pathway is an example of a clinical decision pathway that uses hs-cTn without a risk score to classify patients as low, intermediate, and high risk.92 The High Sensitivity Cardiac Troponin T to Optimize Chest Pain Risk Stratification study enrolled emergency department patients with symptoms suggestive of ACS at eight sites in the US. Using the HEART pathway, three groups were created: rule out, observation, and rule in. Among 1452 patients, 12.7% had 30 day cardiac death or myocardial infarction. In the validation cohort, the hs-cTnT HEART pathway ruled out 37.6%, with a negative predictive value of 99.3%. The rule in group included 14.5%, with a positive predictive value of 57.1%. The hs-cTnT HEART pathway with 0 and 1 hour hs-cTnT has high negative predictive value and moderate positive predictive value for 30-day cardiac death or myocardial injury or infarction.93
A prospective study of patients with acute chest pain compared thrombolysis in acute myocardial infarction, Global Registry of Acute Coronary Events, HEART, and the North America Chest Pain Rule and excluded the components of clinical gestalt. Among 1081 patients (30 day major adverse cardiac events 15.2%), the areas under the receiver operating characteristic curves were 0.809 for thrombolysis in acute myocardial infarction, 0.756 for Global Registry of Acute Coronary Events, and 0.845 for HEART. A thrombolysis in acute myocardial infarction score ≥1 had a sensitivity of 97% and a specificity of 45.7%. A Global Registry of Acute Coronary Events score ≥50 had a sensitivity of 99.4% and a specificity of 7.5%. A HEART score ≥1 had a sensitivity of 98.8% and a specificity of 11.7%. The North America Chest Pain Rule had a sensitivity of 93.3% and a specificity of 51.5%. Without clinical gestalt, the modified HEART score had the best discriminative capacity for 30 day major adverse cardiac events.94 Real time use of the HEART pathway resulted in a non-adherence rate of 20%, mostly due to overtesting. None of these patients had major adverse cardiac events within 30 days. Non-adherence decreased the discharge rate, attenuating the HEART pathway’s impact on healthcare use.95
Do risk scores help identify patients who need additional functional or anatomic cardiac testing after ruling out for AMI on serial hs-cTn testing?
In a retrospective cohort of 1974 emergency department patients undergoing hs-cTnT measurement in two US centers, history, electrocardiogram, age, risk factors scores (not HEART scores, hs-cTnT was removed from the score) were retrospectively calculated from the electronic health record, along with 30 day major adverse cardiac events rates.96 A 0 or 2 hour protocol was used to assess AMI. Patients with hs-cTnT levels above the limit of quantitation (6 ng/L) had an increased risk of 30 day major adverse cardiac events (3.4%) regardless of history, electrocardiogram, age, risk factors score, and patients with hs-cTnT <99th percentile remained at low risk (0% to 1.2%) across all history, electrocardiogram, age, risk factors score strata. These data suggest that hs-cTnT alone is predictive of 30 day major adverse cardiac events without use of a risk score, and that the history, electrocardiogram, age, risk factors score does not reliably identify patients who need advanced cardiac testing. However, the history component of the score was retrospectively abstracted from charts in which clinicians did not record their assessment of the patient’s chest pain in a structured way, calling into question the accuracy of data abstracted from the record representing clinicians’ gestalt. In addition, external validation is needed to confirm the reproducibility of these findings in other patient populations.
Optimal initial management
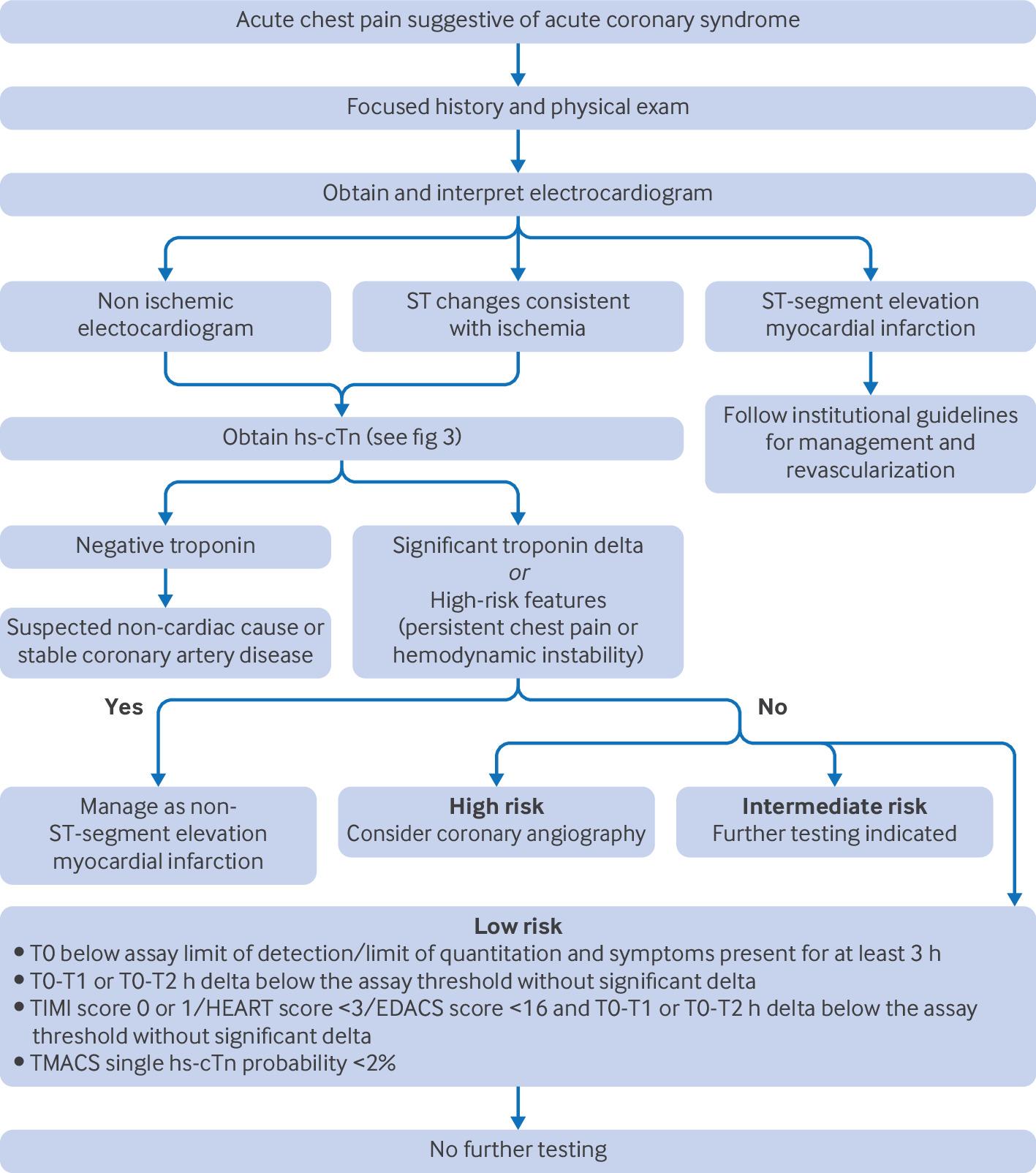
An approach to patients with acute chest pain suggestive of acute coronary syndrome (ACS) is shown in figure 6.

Approach to patients with acute chest pain suggestive of acute coronary syndrome using risk scores for stratification. STEMI=ST-segment elevation myocardial infarction
{kind=link}
High risk patients
For patients with ST-segment elevation myocardial infarction, clinicians should immediately activate the cardiac catheterization laboratory for percutaneous coronary intervention.97 If the clinician is at a non-percutaneous coronary intervention capable center, the clinician should transfer the patient to a center that is capable of performing the test.97 If transfer to a percutaneous coronary intervention capable center is anticipated to exceed 120 minutes, fibrinolytic therapy should be initiated.97 Aspirin 162-324 mg (chewable preferred) should be given.98 A loading dose of a P2Y12 receptor inhibitor (clopidogrel 600 mg, prasugrel 60 mg, or ticagrelor 180 mg) should also be given.98 Anticoagulation should be initiated with a low molecular weight heparin such as enoxaparin 0.5-1.0 mg/kg, or unfractionated heparin 60-70 IU/kg. Enoxaparin might be superior with regard to mortality and complications.99 Oxygen should only be administered to patients who are hypoxic, because routine administration is not beneficial.100 Nitroglycerin and opioids should be given as needed for pain.
For patients with non-ST-elevation myocardial infarction, aspirin 81-324 mg and a P2Y12 receptor inhibitor (clopidogrel 300-600 mg or ticagrelor 180 mg) should be given.101 Anticoagulation should be initiated with enoxaparin 1 mg/kg or unfractionated heparin 60-70 IU/kg.102 As for patients with ST-segment elevation myocardial infarction, oxygen should not be used routinely and pain should be treated with nitroglycerin and opioids as needed.
For high risk patients, defined by new ischemic changes on electrocardiogram, elevated troponins, new-onset left ventricular dysfunction, or other high risk features, the American Heart Association recommends invasive coronary angiography to identify and manage any obstructive CAD. If invasive coronary angiography does not identify an obstructive stenosis that correlates with the clinical presentation and the patient remains troponin positive, cardiac magnetic resonance imaging can also be considered for determining alternative diagnoses.103104
Intermediate risk patients
Current clinical decision pathways have two primary ways patients with possible ACS and a non-ischemic electrocardiogram are classified as intermediate risk. First, the high sensitivity troponin concentration is in the range between the limit of detection and the 99th percentile. These patients have higher cardiac event and death rates in medium to long term follow-up and, as such, warrant further investigation.55105106 Provided that there is not a relevant delta between serial high sensitivity troponin measurements, the patient is not experiencing acute myocardial injury, and can be safely discharged from the emergency department.107In the outpatient setting, patient follow-up for further risk stratification and primary prevention of CAD is indicated to optimize long term outcomes.
Second, the high sensitivity troponin concentration is undetectable or in the range between the limit of detection and the 99th percentile with a negative delta. These patients are classified as intermediate risk using a risk score (eg, HEART). For this group of patients, outpatient follow-up for further risk stratification is also reasonable, though further research is needed to determine the utility of risk scores in determining long term prognosis in the era of high sensitivity troponin.96 We recommend engaging in shared decision making for intermediate risk patients, discussing the risks and benefits of further cardiac testing, including false positives, radiation, and iatrogenic complications.108109
Low risk patients
Low risk patients can be discharged after initial risk stratification. For most low risk patients, urgent diagnostic testing for suspected coronary artery disease is not needed.1 One study of low risk patients found that exercise stress testing had only a modest contribution with a high rate of false positives.110 A study claims that, after ACS is ruled out, the yield of any stress test is very low.111 The most important intervention for low risk patients is addressing modifiable risk factors (eg, smoking cessation, managing blood pressure and lipids) and ensuring primary care follow-up.
Special considerations
Serial troponin testing strategies
Single rule out strategies exist based on a single troponin, 0/1, 0/2, and 0/3 hour pathways. These are guided by published evidence and assay-specific cutoffs, along with approaches to selecting the rule out strategy based on local hospital logistics (see table 6).
Serial troponin strategies in systematic reviews
The European Society of Cardiology 0 or 1 hour hs-cTnT algorithm does not differentiate risk based on whether the patient has known CAD. A subgroup analysis of the Sensitivity Cardiac Troponin T to Optimize Chest Pain cohort included 1430 patients (31% with CAD). Cardiac death or myocardial infarction at 90 days was more frequent in those with CAD than in those without (21% v 10%; P<0.001). Among rule-out patients, 90 day cardiac death or myocardial infarction occurred in 3.4% of patients with CAD and 1.2% without CAD (P=0.09). The negative predictive value was 96.6% (95% confidence interval 92.8 to 98.8) in patients with CAD and 98.8% (97.6 to 99.5) in patients without CAD.46
Occlusion myocardial infarction
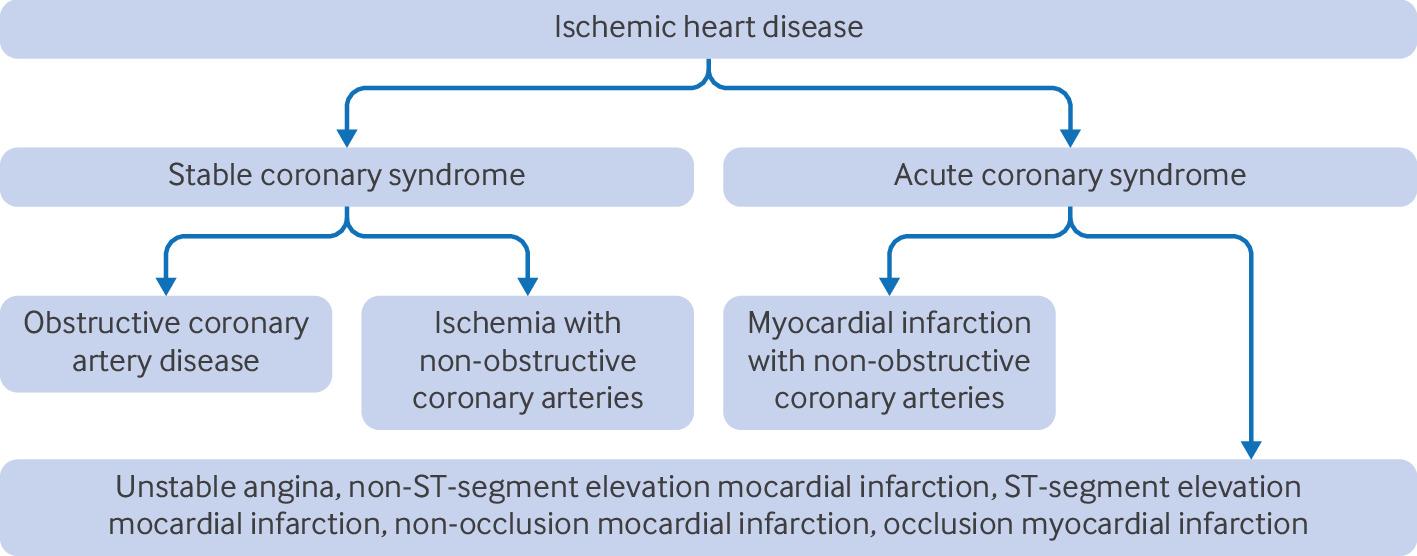
Figure 7 shows the classification of stable versus acute coronary syndrome. Occlusion myocardial infarction refers to type 1 myocardial injury or infarction involving acute occlusion or near occlusion of a major epicardial coronary vessel with insufficient collateral circulation, resulting in imminent necrosis of downstream myocardium without emergent reperfusion. Occlusion myocardial infarction is the anatomic and pathophysiologic substrate of ST-segment elevation myocardial infarction, but not all occlusion myocardial infarction manifests as ST-segment elevation myocardial infarction.113 Patients with occlusion myocardial infarction and ST-segment elevation myocardial infarction have similar angiographic findings, raised cTn levels, and a high risk of pre-catheterization cardiac arrest and index visit mortality. Patients with occlusion myocardial infarction, but without ST-segment elevation myocardial infarction, are less likely to receive emergency cardiac catheterization compared with patients with ST-segment elevation myocardial infarction (38% v 71%).113

Nomenclature and classification of stable versus acute coronary syndrome
{kind=link}
Classifying AMI patients as having occlusion myocardial infarction or non-occlusion myocardial infarction is a paradigm shift providing a nuanced perspective and a broader goal—to recognize all electrocardiogram findings diagnostic of occlusion myocardial infarction—compared with the existing paradigm which aims to identify all electrocardiogram findings diagnostic of ST-segment elevation myocardial infarction. Early identification of patients with occlusion myocardial infarction has the potential to lead to earlier intervention and to improve outcomes in patients with ACS. Further research on emergent reperfusion for non-ST-segment elevation myocardial infarction occlusion myocardial infarction is needed.26113 In non-occlusion myocardial infarction, myocardial injury is due to ischemia but without major coronary artery stenosis. The pathophysiology includes epicardial vasospasm, coronary microvascular dysfunction, spontaneous coronary artery dissection, and coronary thromboembolism. Management requires addressing the underlying cause (eg, antithrombotic therapy for thromboembolism or specific treatments for myocarditis or Takotsubo cardiomyopathy).1114
Ischemia with non-obstructive coronary arteries
One half of patients undergoing elective coronary angiography for possible ACS will have non-obstructive coronary heart disease. These patients are often discharged with a diagnosis of non-cardiac chest pain, and a percentage of them will have recurrent symptoms secondary to cardiac ischemia. Ischemia with non-obstructive coronary arteries can result from coronary microvascular dysfunction or coronary vasospasm, leading to inadequate blood flow to the myocardium. Patients often present with angina-like symptoms, making diagnosis challenging. Diagnosis requires coronary angiography, functional testing, and evaluations of coronary microvascular function and vasospasm. Management focuses on symptom relief through pharmacotherapy, lifestyle modifications, and psychosocial support. Ischemia with non-obstructive coronary arteries is associated with increased cardiovascular risk, necessitating early recognition and management.114115116 Ischemia with non-obstructive coronary arteries and non-occlusion myocardial infarction involve ischemia without large arterial blockages, but ischemia with non-obstructive coronary arteries is focused on chronic ischemia owing to microvascular disease, and non-occlusion myocardial infarction involves acute myocardial infarction owing to other causes such as oxygen supply/demand imbalance in conditions such as sepsis.
ACS presentation in women
Despite declines in cardiovascular disease in recent decades, younger women (<55 years of age) experience increased mortality. Women have a longer time from symptom onset to presentation and are less likely to receive diagnostic testing such as electrocardiogram and troponins.117118119120
In a study of 54 138 patients with chest pain, women were 18% less likely to be triaged as urgent, 16% less likely to be examined by a physician within one hour, 20% less likely to have troponins measured, and 36% less likely to be admitted to a specialized care unit. Women had a 35% higher risk of death in the emergency department and a 36% higher risk of death during the index hospitalisation.121 Another study of 136 247 patients presenting from 1993 to 2006 with ACS (28% women) found mortality rates of 9.6% in women compared with 5.3% in men (odds ratio 1.91; 95% confidence interval 1.83 to 2.00). The authors attributed these differences to clinical presentation and severity of coronary disease.122 Other studies, like a retrospective assessment of the HEART score in 831 women and 1084 men reported a higher risk of major adverse cardiac events at six weeks in men across all HEART risk categories compared with women.123
Women with ACS experience worse outcomes than men, including higher patient and system delays and less aggressive treatment.118 Women have smaller coronary arteries and higher baseline myocardial blood flow, and have different coronary plaque characteristics (more diffuse, non-obstructive, and reduced overall plaque burden). Risk factors like hypertension, diabetes, and smoking, along with non-traditional factors such as psychosocial stress and socioeconomic status, impact women differently. Risks specific to women, including menopause, pregnancy, and hormonal changes, affect cardiovascular risk. Women are more likely to experience microvascular angina, spontaneous coronary artery dissection, and Takotsubo cardiomyopathy.118 Sex-based troponin cut-offs reflect these physiological differences. Historical focus on men in clinical research has led to the exclusion of women from many trials. Current guidelines and risk stratification tools, primarily based on men, could lead to under-treatment in women. Unconscious bias can affect clinical judgment, influencing pain assessment, diagnostic testing, and treatment decisions. Women, especially younger ones, have worse outcomes after ACS and face higher risks of bleeding and complications during revascularization procedures.118
ACS presentation in older patients
Clinicians should have a low threshold for obtaining an electrocardiogram in older patients even in the absence of common cardiovascular symptoms.124 Presentations like falls, syncope, or nausea can be manifestations of ACS in older adults. A study of 558 older adults (median age 83) presenting with ground level fall found elevated hs-cTnT levels in 68.8% and elevated hs-cTnI levels in 15.4%. The incidence of AMI was 0.5%, concluding that falls are not a common presenting feature of AMI and discourages routine troponin testing in this population. However, elevated troponin was predictive of 30 day and one year mortality.125 Owing to the higher prevalence of comorbidities, a thorough assessment is necessary to differentiate between cardiac and non-cardiac causes of chest pain in older patients. The use of structured risk assessment tools ensures that diagnostic testing is targeted to those most likely to benefit.1 In a HEART pathway implementation study, 8474 patients categorized as older adults >65 years (26.9%), middle aged (45.5%), and young (27.5%), revealed that only 7.4% of older adults were identified as low risk compared with 32.0% of middle aged and 51.4% of young patients. The pathway demonstrated high sensitivity (98.8%) for predicting 30 day death or myocardial infarction in older adults, but it did not reduce their hospitalization rates and was associated with increased cardiac testing. The findings suggest that the HEART pathway is less effective at identifying older adults at low risk and has limited impact on their hospitalization outcomes.126
Box 5: What do the patients want their doctors to know?
Patient involvement in medical decision making is an ethical and a legal imperative. Medical decisions are based in part on individuals’ knowledge and acceptance of risk of adverse events.109 In a study presenting a hypothetical scenario to patients with acute chest pain and a group of physicians, 43% of patients preferred discharge, compared with 3% of physicians, with patients underestimating the risks associated with the decision.127 Another survey study demonstrated difficulty with risk estimation,128 and substantial variation in patients’ reported tolerance for adverse events from emergency department chest pain.129130 A cross sectional study on patient preferences for diagnostic testing in the emergency department demonstrated patient preferences differed noticeably across levels of risk, benefit, and cost of diagnostic testing. Cost was the strongest and most consistent factor associated with decreased desire for testing.131
A survey conducted in patients with low risk chest pain presented a hypothetical value for the risk of adverse outcome that could be decreased by hospitalization and asked them to identify the risk threshold at which they preferred admission versus discharge. Measurement of patients’ risk tolerance or methods of shared decision making not dependent on assessment of risk tolerance is needed.128
The European Society of Cardiology guidelines recommend patient-centered care by assessing and adhering to individual patient preferences, needs, and beliefs, ensuring that patient values are used to inform all clinical decisions. The guidelines recommend including patients in decision making and informing them about the risk of adverse events, radiation exposure, and alternative options. Decision aids should be used to facilitate the discussion, and patient discharge information should be provided in both written and verbal formats before discharge.87
One patient with lived experience of chest pain and multiple presentations to the emergency department emphasized the following key points regarding care for individuals with chest pain:
-Coordination of care: It’s important to clearly define responsibilities between healthcare providers and patients. This includes organizing tests, sending in results, and ensuring proper follow-up (ie, who follows up on a stress test result). Knowing what to expect in the emergency department visit and after dismissal was important to patients.
-Quality of life: The impact of treatments, particularly medications, on daily life should be discussed. For instance, one patient highlighted how beta-blockers and blood thinners affected their quality of life by increasing their fear of falling, or how beta-blockers increased dizziness.
-Cost and convenience: Consideration of the financial burden and time required for treatments is important to patients. Patients want to be informed about costs, insurance coverage, and the practicalities of accessing care, especially in rural areas.
-Clear communication: Healthcare providers must ensure that patients fully understand the risk, benefits, and alternatives of the medical decisions, including long term effects and potential side effects of medications. Patients highlighted the importance of discharge instructions to understand what had happened in the emergency department encounter, and what to do if the chest pain returns.
These points emphasize the importance of patient centered care, where communication, understanding, and flexibility are prioritized to improve overall treatment experiences.
Emerging treatments
Advances in pre-hospital alert systems, point of care troponin assays, wearable devices, shared decision making, non-invasive imaging strategies, artificial intelligence, and big data applications promise to improve management of patients with chest pain.132
Artificial intelligence and precision medicine
Artificial intelligence and machine learning tools are being developed to enhance risk stratification and guide clinical decision making. These technologies can analyze large datasets, including patient history, biomarkers, and imaging results, to predict outcomes and optimize treatment strategies. Recent research has also begun to explore the role of using artificial intelligence to detect regional wall motion abnormalities on point of care ultrasound.133134 This offers a promising role for detecting subtle signs of myocardial injury not captured via electrocardiogram or visual assessment, but it must be used with caution as accuracy can vary across algorithms and devices.135
A review of machine learning in stress electrocardiogram improved sensitivity and specificity to over 96% and reduced false positives by up to 21%. Natural language processing also helped categorize stress echocardiography reports with nearly 98% accuracy.136 A study comparing artificial intelligence recommendations with cardiologists’ decisions for 102 patients found good agreement for patients with high and low risk chest pain, but less agreement for patients with intermediate risk chest pain.137
Point of care devices
New devices that provide rapid access to vital signs and electrocardiogram data before first medical contact are being explored. These tools aim to improve the speed and accuracy of ACS diagnosis and management. Point of care troponin testing devices are undergoing clinical trials with the aim to accelerate clinical decision making, improve emergency department efficiency, and reduce unnecessary hospital admissions. Point of care testing might be especially beneficial in settings that are remote or have limited resources, including pre-hospital settings.138
Guidelines
Clinical guidelines aim to summarize the best evidence and guide practice while decreasing practice variability. Guidelines for acute chest pain have the potential to shorten emergency department length of stay and time to diagnosis, reduce practice variation and standardize the use of serial biomarker, cardiac risk stratification, and advanced cardiac testing.
The most current guidelines are the European Society of Cardiology guidelines for the evaluation and management of acute chest pain.87 These guidelines emphasize a structured approach incorporating diagnostic pathways, timing of serial troponin measurements, and risk stratification. They recommend the use of the 0/1 hour or 0/2 hour hs-cTn algorithms for the rapid rule out and rule in of non-ST-elevation myocardial infarction.47139140 Critiques to this algorithm include that it does not differentiate risk based on known CAD.46 Supporters of the algorithm report that it is helpful even in patients presenting early (defined as within 3 hours of chest pain).141 Changes in the 2023 version include the consideration of using coronary computed tomography angiography or a non-invasive stress imaging test as part of the initial workup in patients with normal hs-cTn, no electrocardiogram changes and no recurrence of pain (previous guidelines recommended testing).
Table 7 summarizes the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain emergency department recommendations.1 Changes in this guideline include that patients with a low (<1%) risk of death or major cardiac events within 30 days do not require stress testing or cardiac imaging. Previous guidelines recommended non-invasive stress testing within 72 hours for all patients presenting with acute chest pain. Also, for those at intermediate risk and no known coronary artery disease, the decision to use anatomical or functional advanced cardiac imaging after a negative ACS workup should be guided by local availability, expertise, and patient preference.
Summary of clinical guidelines for approach to patients with chest pain in the emergency department
The American College of Emergency Physician Clinical Policy on valuation and Management of Patients with Suspected non-ST-elevation myocardial infarction and Guidelines for Reasonable and Appropriate Care in the Emergency Department-1 guidelines from the Society of Academic Emergency Medicine are summarized in table 7.142 Guidelines for Reasonable and Appropriate Care in the Emergency Department-1 guidelines are focused on patients with recurrent low risk chest pain and add that if a previous imaging or stress test is reassuring, a single troponin value below the validated threshold is enough to rule out ACS. Similarly to the European Society of Cardiology, these guidelines recommend screening for depression and anxiety among those with recurrent emergency department visits for chest pain and negative workup.9
Both the American Heart Association/American College of Cardiology guidelines and the European Society of Cardiology guidelines recommend a risk based approach to angiography with early invasive strategies for patients at high risk including those with ongoing chest pain, dynamic electrocardiogram changes, hemodynamic instability, or life threatening arrhythmias.
Conclusion
Chest pain is a common complaint in emergency departments worldwide. Ruling out ACS and other life threatening conditions is a cornerstone of emergency medicine practice. The initial evaluation includes an electrocardiogram, and a minority of patients with ACS will have ST-segment elevation myocardial infarction. An ischemic electrocardiogram is useful for ruling in ACS, but a non-ischemic electrocardiogram is not useful in ruling out the diagnosis. The remainder of these patients have non-ST-elevation myocardial infarction, unstable angina, or non-cardiac chest pain, and differentiating between ACS and non-cardiac chest pain is the next step. Initial and serial high-sensitivity troponin measurements, combined with structured risk assessment tools such as the HEART score, help clinicians identify patients who require further investigation and guide appropriate management. In patients at low risk, routine diagnostic testing is unnecessary, and the focus should be on addressing modifiable risk factors and ensuring appropriate follow-up. For patients at intermediate and high risk, further testing, including cardiac imaging, might be necessary to rule in or rule out ACS and guide treatment decisions. Patient involvement in decision making is crucial, with a clear discussion of risks, benefits, and alternatives to facilitate informed choices. The interpretation of high-sensitivity troponin levels should be nuanced, acknowledging that elevations could indicate conditions other than ACS. Proper follow-up and management of these patients is essential to improve long term outcomes. Overall, the evaluation of chest pain in the emergency department should be guided by an evidence based approach that prioritizes patient safety, minimizes unnecessary interventions, and optimizes clinical outcomes.
Key questions that future research needs to answer
-What are the optimal diagnostic pathways for patients with intermediate risk chest pain, and how can these pathways be improved to reduce unnecessary testing while maintaining high diagnostic accuracy?
-How can sex-specific differences in ACS presentation be better integrated into clinical decision making tools to improve early detection and treatment outcomes for women?
-What is the clinical utility of integrating artificial intelligence and machine learning models with high-sensitivity cardiac troponin testing in the emergency department for predicting adverse cardiac events?
-How can the management of patients with elevated troponin levels but no evidence of obstructive coronary artery disease (eg, ischemia with non-obstructive coronary arteries and non-occlusion myocardial infarction) be optimized to improve long term cardiovascular outcomes?
How patients were involved in creation of this article
We discussed this article with a patient with lived experiences and who had presented to the emergency department several times as a patient and as a caregiver. They have experience in both the US and UK healthcare systems. They stressed the importance of clear coordination of care, where responsibilities between healthcare providers and patients are well defined, particularly regarding organizing tests, reporting results, and follow-up. They highlighted the need to consider the impact of treatments on quality of life, including the practical and emotional effects of medications (ie, starting beta blockers or anticoagulants); the importance of addressing cost and time involved, ensuring patients are informed about financial and logistical aspects of their care and the importance of clear dismissal instructions.
Also, three of the authors worked with patients with lived experiences of chest pain during the writing of a clinical guideline for management of low risk chest pain. Their voices are reflected in box 5.
Acknowledgments
We thank Dr Colin O’Shea for providing the electrocardiograms included in this manuscript, Ms Dana J Gerberi, MLIS for conducting the literature search, and Ms Trish Sarson for sharing her experience in the healthcare system.
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: MT received research funding, honorariums and consultancy fees from Abbott, Beckman, Ortho-Quidel, Radiometer, Roche, and Siemens. RB received research grants from Siemens Healthineers, Roche Diagnostics, and Abbott Point of Care, and has consulted for Roche, Siemens, Abbott, Beckman Coulter, Singulex, Creavo, Aptamer Group, LumiraDx, and Radiometer.
Provenance and peer review: Commissioned; externally peer reviewed.